
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › cold sore treatment
- This topic is empty.
-
AuthorPosts
-
Robert GreggParticipantHi Ron,
Cold sores/fever blisters/HSV-I tend not to return to the same site about 90% of the time.
Canker sore/aphthous ulcers are more like 50%, with the deeper, crater-like ulceration sometimes needing to be surface ablated and with a new wound to cover or seal it. In rare instances, you have to burn it out to the basement membrane. I’ve done that twice in 12 years….once on my wife.
Tongue lesion are much, much better in their resolution and recurrence rates….more like cold sores.
Bob
RodSpectatorRon,
Typically, the lesions you discribe are not viral. They’ve been linked to an immunological problem as of late, but nothing definitive.
Often there is a ‘trigger’ for these. Some speculation that there is a food ‘allergy’ or ‘sensitivity’ involved in the ‘trigger’.
And they CAN hurt like a ‘S.O.B.’!!!
One thing that I’d have her do is switch to a non-SLS toothpaste. Sodium Laryl Sulfate is the detergent in toothpaste that causes the foaming that we all love to feel when we brush. But it can denature proteins and also has an effect on the lipids in the oral tissues.
It’s felt that this can, in a high percentage of canker sore sufferers, make them more susceptible. Some patients are not helped whatsoever by using an SLS-free toothpaste, and some are helped tremendously.
She should keep track of foods she eats, and switch to an SLS-free toothpaste. Put it this way — can’t hurt to try.
What laser did you use to treat the lesion.
I usually first treat it with my diode, followed immediately by the Waterlase.
Rod
whitertthSpectatori used my waterlase at .75 watt no air or water…. she seemd to have a very high recurrence rate of all her ulcers…..
Robert Gregg DDSSpectatorRon–
Canker sores/aphthous ulcers often need to have the lesion a”altered”at televel of the basement membrane.
Since the Waterlase is such a shalow penetrator that ought to work the best to do so w/o anesthesia.
Near infrared lases–810 and 980 diodes and 1064 pulsed Nd:YAGs are deeper penetrators and effect the recurrece rates by “bio-modulating” the deper tissues surrounding the clinical appearing lesion.
Bob
N8RVSpectatorQUOTEQuote: from Robert Gregg on 8:09 pm on April 9, 2003
Hi Ron,…Canker sore/aphthous ulcers are more like 50%.
Hmmm … as a new laser user, this is disturbing. I attended a seminar and was told that the use of the Er:YAG laser on RAU offers “immediate relief from pain, healing in a couple of days and THE ULCER WILL NEVER RECUR IN THE SAME SPOT.”
Big difference in “never” and “50%.”
Relief from cancer sores was a real draw for me — I see them all the time and would love to offer a definitive treatment for them. However, I’ll be somewhat reluctant to charge for a procedure that only works half the time.
Thoughts from other users …?
(Edited by N8RV at 4:10 pm on May 3, 2004)
Robert Gregg DDSSpectatorQUOTEQuote: from N8RV on 4:08 pm on May 3, 2004QUOTEQuote: from Robert Gregg on 8:09 pm on April 9, 2003
Hi Ron,…Canker sore/aphthous ulcers are more like 50%.
Hmmm … as a new laser user, this is disturbing. I attended a seminar and was told that the use of the Er:YAG laser on RAU offers “immediate relief from pain, healing in a couple of days and THE ULCER WILL NEVER RECUR IN THE SAME SPOT.”
Big difference in “never” and “50%.”
Relief from cancer sores was a real draw for me — I see them all the time and would love to offer a definitive treatment for them. However, I’ll be somewhat reluctant to charge for a procedure that only works half the time.
Thoughts from other users …?
(Edited by N8RV at 4:10 pm on May 3, 2004)
I wasn’t very clear. The 50% refers to near IR lasers that are deep penetrators and the observation that aphthous ulcers as opposed to HSV-I require a surface eschar from a laser to achieve 90% plus non-recurrance.
It is a good idea to be skeptical of any claims of 100% for anything. 90% is a very significant amount of resolution. Anyone out there telling patients RCTs are 100%?
Here’s what you can do:
Charge whatever you feel is a fair fee to “eliminate” all recurrences of the lesions you want to treat in a specific location, guarantee to the patient the lesion will not return to the same location, offer a full refund or retreatment at the patient’s discretion if it should do so. I have never had to refund any $$. (How’s that “never” working for you now?) All but a few “recurrances” have been lesion appearaces in a new location.
Hope that clarifies my previous post, and addresses your concerns over absolute results.
Wlecome to the laser family!
All the best,
Bob
kellyjblodgettdmdSpectatorI think this thread brings out an interesting issue in laser dentistry (or general dentistry, for that matter). The “I heard it in a seminar so it must be true” issue.
Make no mistake, lasers are great for treating soft tissue lesions. However, to believe that anything is 100% successful just doesn’t seem logical.
I run into this problem frequently with new laser users and receive many phone calls (referred to me by my laser rep) with questions such as: “How come my patients jump when I’m trying to do a filling. I don’t think this laser anesthesia thing works. The laser rep told me it should be a piece of cake.”
As we all know, often times these claims are true, but so much of that success is based on good clinical decision making. And it’s hard to make good clinical decisions without some good experience or training.
If I could make a suggestion to N8RV, learn laser physics like the back of your hand, and then you’ll know exactly what your laser can and cannot do. Don’t believe the hype!
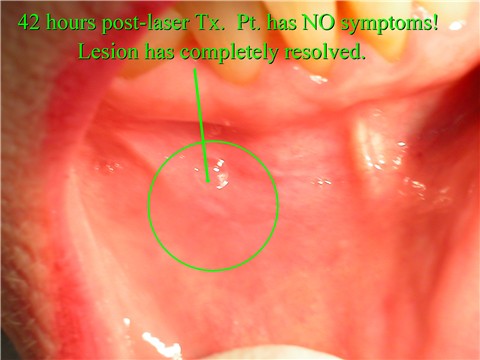
Here is an example of a lesion I treated w/ Nd:YAG about one year ago. It has not yet returned.

Kelly
Robert Gregg DDSSpectatorKelly,
Very good advice.
Very nice treatment. I am impressed!
Ron S is wondering how come I couldn’t do this for him!
 Shooot! Sorry Ron!
Shooot! Sorry Ron!Bob
N8RVSpectatorThanks for the clarification of the 50%-thing.
And, Kelly, thanks for the pics and explanation. I’m attending the DELight training seminar this weekend to get some good experience and certification and willl be eager to put some of it to work next week!
Thanks again,
Don
-
AuthorPosts