
Forums › Erbium Lasers › General Erbium Discussion › Crown lengthing closed and opened.
- This topic is empty.
-
AuthorPosts
-
dkimmelSpectatorThis is a crown lengthening case I did today. Figured Danny has too much free time on his hands. Needed to keep him out of trouble..
This is a 78 Y/O wt male. He is one of my typical Florida cardiac patients. Working with maybe 50% of his cardiac capacity. We are doing some heroics. He has a lower RPD, that was held in place by an over denture attachment on the right and splinted 22×21 with an attachment. His OH is lacking and recurrent decay caused 21 and 22 to fail. What we are going to do is place an attachment on 21 and 22 as was done on 28. In oreder to do this Cl is required. I did this case as a closed procedure and then opened the case to see how it looked. I have been training my assistant to take the pictures and things did not go a swell as expected. However, you can get a good idea on how things went.
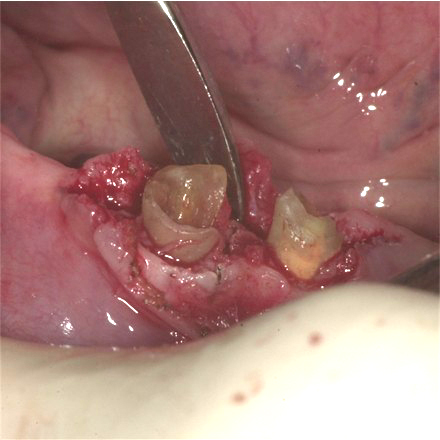
1. This is an occusal view of 21 and 22.
2. Buccal view.

3. Attachment on #28.

4. 3 mm sulcus.

5.Limited attachment on #21. Evaluate the attachment post sx and then deal with the need for grafting at a second sx.

6.#22has a thick ridge of bone and plenty of attachment.

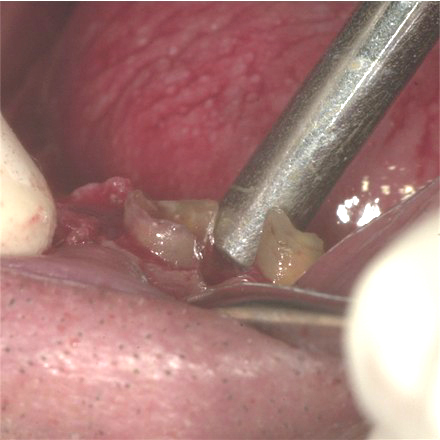
7. Z-4 tip 1.75 W 70A 30water to 5mm around tooth #22 trying to blend. On #21 only the lingual was done blending to the interprox . areas using the G-6 tip.


8.The Diode was used to remove 2mm of tissue around #22 and on the lingual of #21.
1.5 W continuous.
9. What was left was a nice trough around #22. This was leaving a osseous defect on the distal and there was also a very thick ledge of bone on the buccal with a trench between it and the tooth. You can not see the lingual of #21 but it was more acceptable with a thinner edge of bone. The nice little area of char was in several places. This was not from the diode but the Z-4 tip. I was careful to keep the tip out of contact but it was not always possible.
10. this is the best picture I have. This is after recontouring the bone. Removing the thick ledge of bone, the troughs and trying to recontour the interprox. areas between 21 and 22 .
11. Here we are done.

It was interesting see what was left after doing a closed procedure. I believe if I had not opened this case it would have failed. My concerns are with the troughs left around the #22, the inability to contour the interprox area , leaving a thick ledge of bone on the buccal and the char areas of bone where the tip contacted the bone. The lingual of #21 was acceptable and I was able to blend to the distal but not the mesial. The use of the G-6 tip was part of the reason the lingual worked out better. More likely it was because the bone was a thin plate. I still had to currette a thin skin of bone off the lingual of the root on #21.
I had no problem finishing off the case after it was opened. It is much easier using the laser when you can see what you are doing.(Edited by dkimmel at 6:57 pm on May 26, 2004)
-
AuthorPosts