
Forums › Erbium Lasers › General Erbium Discussion › Er:YAG laser for gingival recontouring
- This topic is empty.
-
AuthorPosts
-
Glenn van AsSpectatorHi folks: Sorry for the delay in not posting but I am slowly recovering here at home. Here is a case I recently completed for a lady. I am only showing you the maxillary arch but we have now completed the lower arch as well. I was unable to get her to pose for the facial profile so all I have is scope shots for the procedure.
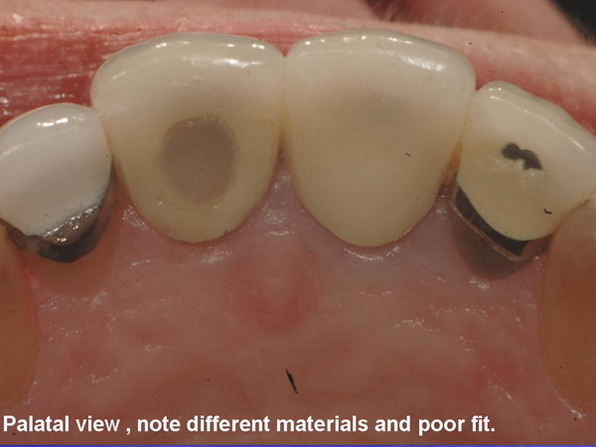
Her chief complaints were that the color of the crowns all done at different times made the teeth not look uniform in shade. In addition she mentioned that she didnt like the fact that the crowns looked “square” and that the gingiva was higher on the canines than the centrals and laterals. Finally she didnt like the roots showing at the edge of the porcelain on the centrals.
We discussed making the teeth longer incisally versus at the gingiva (she does show some tissue when she smiles) to take away the squareness of the teeth. Tarun and company talk about the ideal of 75-80% of the width vs length in incisors and others have talked about the central being 10.5mm and working from there.
This ladies centrals were 8.75mm long but she didnt like the temps which were 10.5 so we made a compromise of 9.75mm in the end which was longer than her originals but shorter than temps which phonetically and esthetically looked too long.
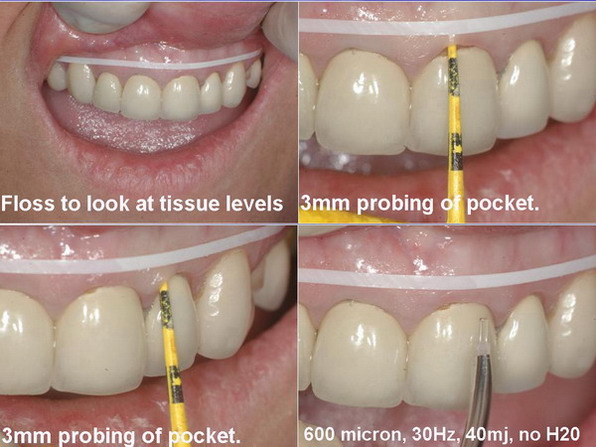
In deciding that some of the increased length could come in her case from altering tissue heights, there came a decision to probe the pockets and if necessary to sound to bone). In probing the maxillary centrals and laterals the probing depths were 3-4 mm so to increase length gingivally by 1-1.5mm was not alot. If the lower arch osseous surgery (open flap ) was used to alter the length because the pockets were only 1-1.5mm and rebound if only soft tissue was altered could be expected.
I have found that dental tape (Teflon floss) can be a great tool to use on dry tissue to guide you as to your approximate gingival zeniths and gingival height of contour. A black sharpie is also helpful. When I demonstrated to this patient that the upper centrals should match with the canines (gingival zenith ) and that the laterals should be 1/2- 1mm shorter, she mentioned to me that she would like them to be the same (easier for me!!).
I have showed in the photos on recontouring a couple of things……
1. a 600 micron tip was used initially to remove some tissue and on healthy tissue this can be done without much fear of bleeding.
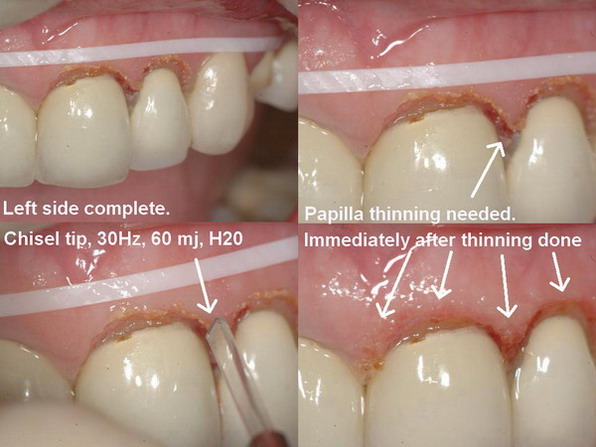
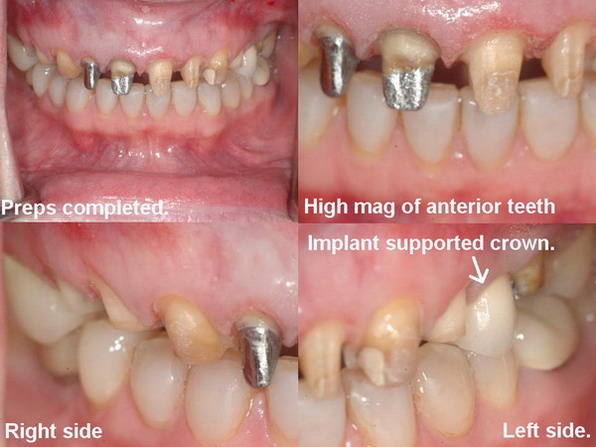
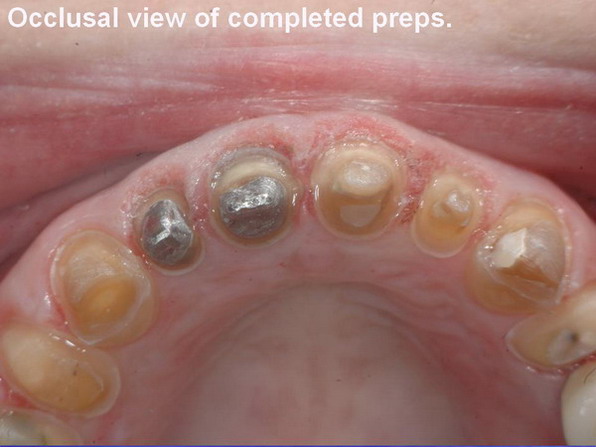
2. a chisel tip can at the right angle be the perfect tool for bevelling down the tissue and creating a nice papilla with knife edged margins.The preps were done the same day and then temps placed. The original reason for composites facially and the crowns was the moderately severe tetracycline staining that was present on the teeth. The diode laser at 0.7w, 10Hz was used for careful troughing for the impression. Intermittent appointments for Baked Bisque tryin (she was very nervous about color) and also the final insertion photos were not shown to decrease number of photos.
The final photos are at 3 week healing photos and prior to the lower arch (now healing) being completed.
In looking cricially at the case I think that some rebound occurred on the right central but that all in all the case is a big improvement (patient is happy) over the initial status.
I wanted to show you that when we start evaluating the results in the “throwaway” journals that we receive monthly, start critically looking at the Gingival Heights of contour, the shape and heights of the tissue for symmetry and improvements that could have been done. Was it severe that it needed an open flap, was it minor that it could have been done with a diode or as in this case the erbium. I always found myself concentrating on the whites, the color improvement, the instant orthodontics, the incisal edges, but if we concentrate on the PINKS and how they interact with the whites, we might begin to see how lasers can really be used effectively to help us in our cosmetic cases.
In closing, I am far from a cosmetic guru, I am just a GP who occassionally gets a chance to treat cases like this that bring pride and enjoyment to me at the end. Is it perfect…….nope, but its a pretty good result, and hopefully teaches a few out there to look at the Pinks not just the Whites!!
PS I know that in the postop shots she isnt occluding in CO but is forward edge to edge. I didnt catch that when I was photographing it through the scope. Will try to get some post op shots with the floss for my own benefit and also some shots of the healed lower in CO as it exists now.
Cya
Glenn

https://www.laserdentistryforum.com/attachments/upload/Slide5 edited_resize_resize.jpg” border=”0″>







(Edited by Glenn van As at 4:53 pm on Mar. 25, 2005)
dkimmelSpectatorGlenn I am not sure I understand photo #1. Can you explain that one again. Oh and what pain meds do they have you on? They must be pretty good by the looks of the photos.

Andrew SatlinSpectatorHi Glenn,
I don’t see any photos?
Is it just me?
Andy
Glenn van AsSpectatorI have asked Ron to put the photos (actually uploaded to his server twice back into the post, because due to password issues they werent posted with the original thread)……I hate to upload them again.
If he doesnt do it in a day or two I will put them on the post again.
Glenn
dkimmelSpectatorSure Glenn we believe you!! Take it easy, relax and get better.
AnonymousGuestGlenn, I deleted the images from the server. I think the problem was the names of the images. Can’t have any _ or spaces. Go ahead and respond to your own post and upload the images again with names not having _ or any spaces.
thanks!
2thlaserSpectatorDavid,
I think it’s the Canadian version of photos, eh?…Glenn, you just get better ok? Don’t worry about the photos, we can see them in our minds eye! Just kidding of course. We really just want our Glenn back online and in living color. Really, no one posts as well as you do. Thanks for the sharing!M
Glenn van AsSpectatorAlright the photos are in and I can sleep again…..sheesh!
Just kidding, now hopefully there will be some discussion over this case. I know that Osseous recontouring continues to be a huge area of debate.
This was only soft tissue not bone.
Cya
Glenn
Andrew SatlinSpectatorHi Glenn,
Nice before and afters!
This does look like a good candidate for osseous judging from your preop probings. Why only soft tissue?
Andy
Glenn van AsSpectatorHi Andy, when I measured the probings were 3-4 mm on the facial and I wanted around 1.5mm. I felt I didnt need any extra with the osseous.
Do you feel different?
Thanks alot for the kind words.
Glenn
Andrew SatlinSpectatorGlenn,
I suppose time will tell. 1.5 mm seems like minimum but it depends on the patient.
Have you seen much rebound on cases in the past?
I have definitely treated patients with gingivectomy and not had problems. I am now doing more osseous using Danny Melkers flap design and philosophy and enjoying the results!
See ya
andy
Glenn van AsSpectatorAndy, I too have learned alot from Danny. This patient actually had open flap on the lower but not the maxilla.
I actually like the results on the maxilla more but my error was that the staff thought I was doing the same on the lower arch as the maxilla and scheduled the patient for 4 hours of preps 1-2 weeks after the open flap. Tissue hadnt healed, I still went ahead, and now suspect that the lower arch may need a graft on the lower anterior. My surgical skills still dont rival many out there yet but I am trying to improve.
ALl the best and to be honest there is so much stuff coming out right now on laser assisted closed flap osseous that its mind boggling. I had a guy give me a bad time after the last Nash Institute telling me he was doing closed flap for everything and had zero problems and was wondering why I was recommending so much open flap with the laser for multiple teeth or multiple surfaces…….
Goes to show you I have come along way from yours, Hack2 and Dannys pushing.
Still not there yet but getting there!!
Glenn
-
AuthorPosts