
Forums › Erbium Lasers › General Erbium Discussion › Revisiting a case
- This topic is empty.
-
AuthorPosts
-
Glenn van AsSpectatorHi folks: Part of this case was lost when the server went down so here it is completed now to the crown prep phase.
Danny, I thought lots about whether to do closed or open here so please dont think that you are not having an effect on stressing the Biologic principles here. I felt that I only had one mm or 2 at the most to remove in such a small area that I chose to do closed CL.
This is a case which I had alot of experience on because Danny had told me that my other case wouldnt work. I took some of what Danny said to heart and wanted to show you a case that we just completed the endo (sorry I forgot the radiographs).
This case is a lady who has never had a crown but needs 20 teeth done because of huge amalgams.
Finally convinced her to have this one done because of decay under the old amalgam.
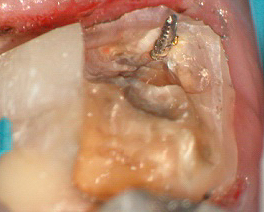
On cleaning out the amalgam I encoutered the decay going into the pulp on the distal buccal.
Now last time I had a case like this I got grilled because I left a buildup intact and this time I removed it in part one and opened the tooth.
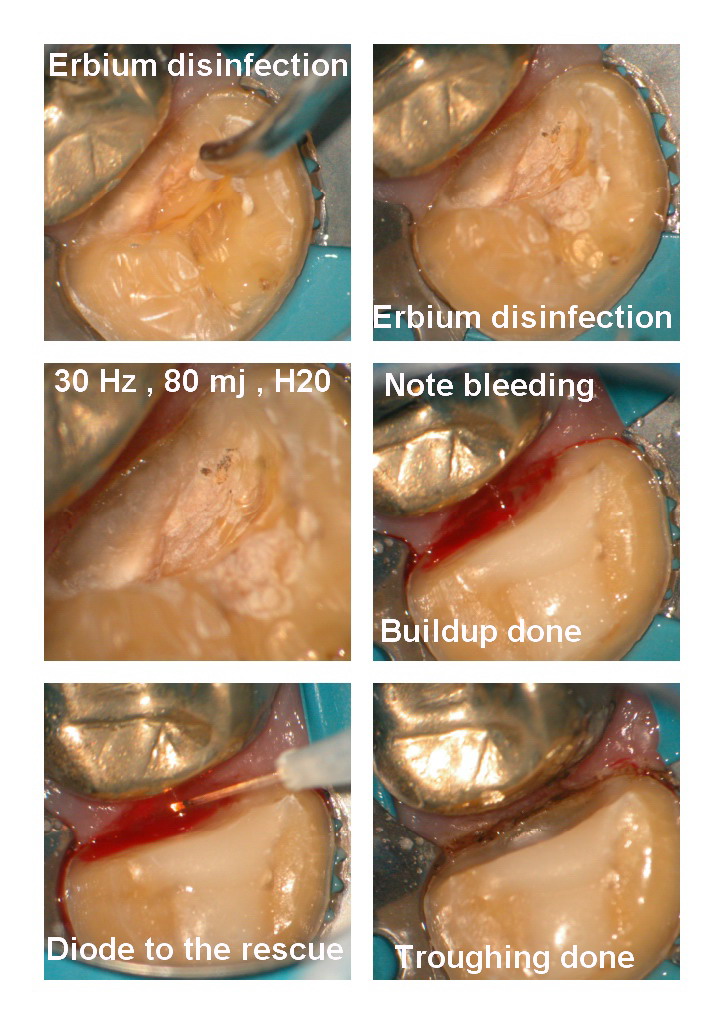
Yesterday I obturated it and when I troughed with the diode for the impression there was one spot on the buccal where there wasnt enough BW to get a good impression. At high mag you can see and feel this with the diode because it will not trough (its running into the base of the pocket), now this area was around 2-3mm in width right at the furca.
I decided at the time to just gently reduce this area by 1-2mm with the erbium to get a margin for the crown.
Now Danny, lets see how this heals. One concern I had was that the margin was quite thick and if I did your root reshaping I might have to take ALOT off.
ANother concern with raising a flap was getting into the furcation. I will say that I needed good magnfication and really took of very little (not circumferential)
I was pretty pleased that I saved the tooth after completing the 5 canal molar endo ,post, Build up and crown prep I relined the temp.
Hope you enjoy the case and discuss the merits of what I did here in a civil fashion.
I recently did do a case which I shot on video that had troughing in the bone after closed CL on the interproximal that I Cleaned up after raising a miniflap, but this one was just on the buccal and I decided to treat it this way.
I will show the healing when it comes back.
Glenn





HERE are the photos from Visit 2…….


AnonymousGuestGlenn, great images. What power mag?
Glenn van AsSpectatorHi Ron : Most are 10-16X mag. I have found through trial and error than anything below 10X mag does get the viewers attention because in using a regular SLR camera you can get that close.
Now I never crop the image or zoom in on it, so the image is the actual size you are seeing. One problem with using say no magnfication and then taking a camera and shooting a pic and zooming in on it, is that the magnification of the picture is not what you were seeing it at. Of course all sorts of things jump out at you then like excess resin in places you dont want, margins that looked chipped or incomplete or anatomy on your resins that isnt in the right spot.
These were some of the things I noticed when I first started using the scope and shooting some of my old work……..(that wasnt alot of fun!!)
Anyways, I just wanted to show you that in this case the margin wasnt quite clear on the buccal after the diode and I was at the end of the pocket (I can feel and see that I cant go any deeper ) and therefore I chose to just make a mm of adjustment in that area to allow for a clear impression.
Glenn
ASISpectatorHi Glenn,
Very good effort again to show the progress of a case.
Did you leave the pin in?
The closed osseous ought to work fine here.
Andrew
Dan MelkerSpectatorGlenn are you sitting down!
I have no problem with what you did at all. It appears there is sufficient space between your troughing and the bone-BW was not in violated at all! Correct me if I am wrong but you did not touch the bone interprximally.
Think of gingival currettage burs except far better with the laser! If there was no troughing of the bone this case will be highly successful!
Glenn as far as the furcation, when I raise a flap it is usually protected by a split thickness flap. I can usually reshape a problem with no effect what so ever on the health of the furcation. But frankly that is another topic.
The indications for your procedures in this case are ideal and beautifully done.
It really is incredible how you can show your cases and I am truly enjoying seeing them!
Thanks for the post and great case!
Danny
Glenn van AsSpectatorDanny I am sitting down……phew.
I just finally finished my Dental Clinics of N. America chapter this weekend and had a drink. Gosh it was a hard thing to do.
In any event thank you so much for your kind words. IT does make a world of difference to me. In writing the final words of my chapter I resoundingly told people to please consider biologic principles in considering when to do closed crown lengthening and your words of wisdom were ringing in my ears.
I do believe that eventually we will figure out when to do closed with the laser and when to flap. I myself still believe that there is a role for CL of a closed flap variety but not some of the crazy stuff I see posted on the net.
I have come to at least consider when is it possible and not blindly fall into it.
I want to thank you for your kind post, and I am sure that you must at times shake your head with some of the posts here (including mine) but I think with time like in so many things we gradualize towards a common area where we both give a little and find some common ground.
I know that you have made significant attempts to open your mind and eyes to some new ideas includin LPT and this closed crown lengthening and you in doing so have made me think alot about flaps and when to do them.
THanks for your input on this and I hope to gradually get to a point where people say……..hmmmm….that is how to do it. I am far away from there now but getting closer all the time.
Thanks again Danny……..
Glenn
kellyjblodgettdmdSpectatorGlenn – Nice post. Man, that’s a great set of pics! I do have a question that may seem silly, but with all the work provided to save #30, has this patient seen the value in treating #31 at the same time? That “wrap-alloy” is another time bomb waiting to blow (fractured cusp in future, no doubt at some time).
With the magnified pictures, do your patients have an easier time accepting more “comprehensive” Tx plans?
Just curious. I know that with so many of my patients that are more driven by their insurance benefits, the root canal, CL and crown would well exceed their benefits for one given year. Was that an issue here?
Thanks for the effort on this one. It’s really well put together. And congrats on finishing the Chapter. That’s got to be a monkey off your back. When is that issue coming out?
Kelly
Glenn van AsSpectatorHi Kelly: First off I want to compliment you on your always upbeat posts. They are a great reflection of the person I saw at the ALD who seems always positive…….thanks.
Kelly, I am trying to get away from this one tooth mentality that I have been saddled with and treat more comprehensively.
This patient if you look at the radiographs has a tremendous number of large amalgams.
I have never been able to convince her to have anything replaced if it aint broke or decayed. This is her first crown and only because the tooth was a little sensitive.
I totally agree with you about #30 and there are more besides this one.
THe patients are more likely to do the dentistry and less likely to complain about deep fillings that are sensitive.
The magnified images on video to the TV and also through pics on the camera help a huge amount.
Here is a case I did today………sorry no pics but the patient again is in a position where he needs some more work but we are starting with the tooth with decay.
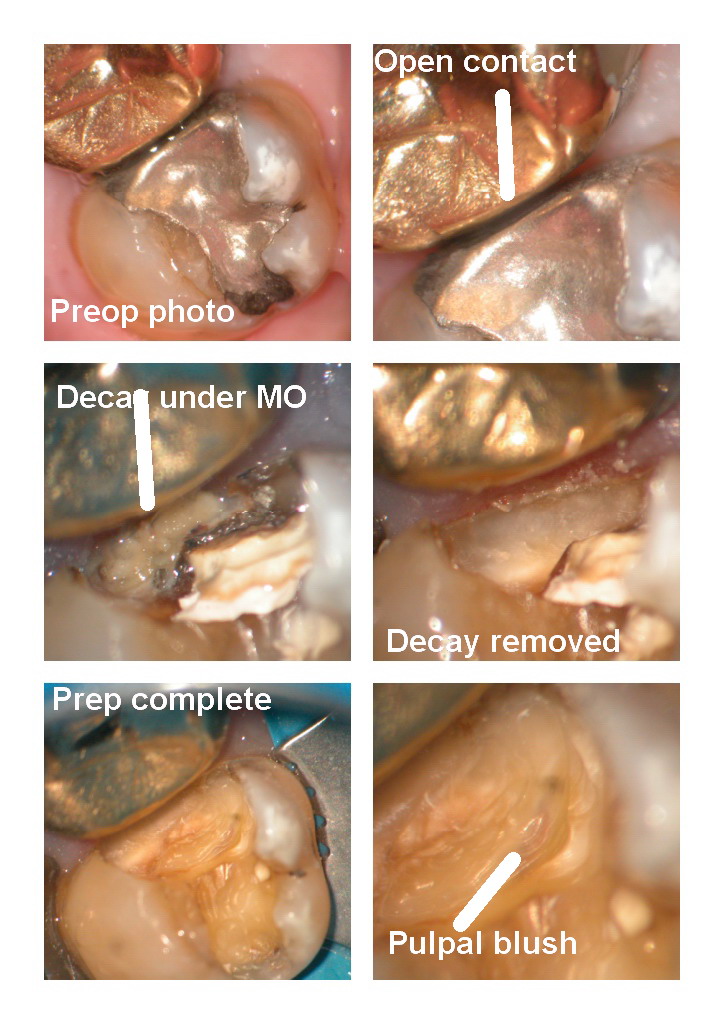
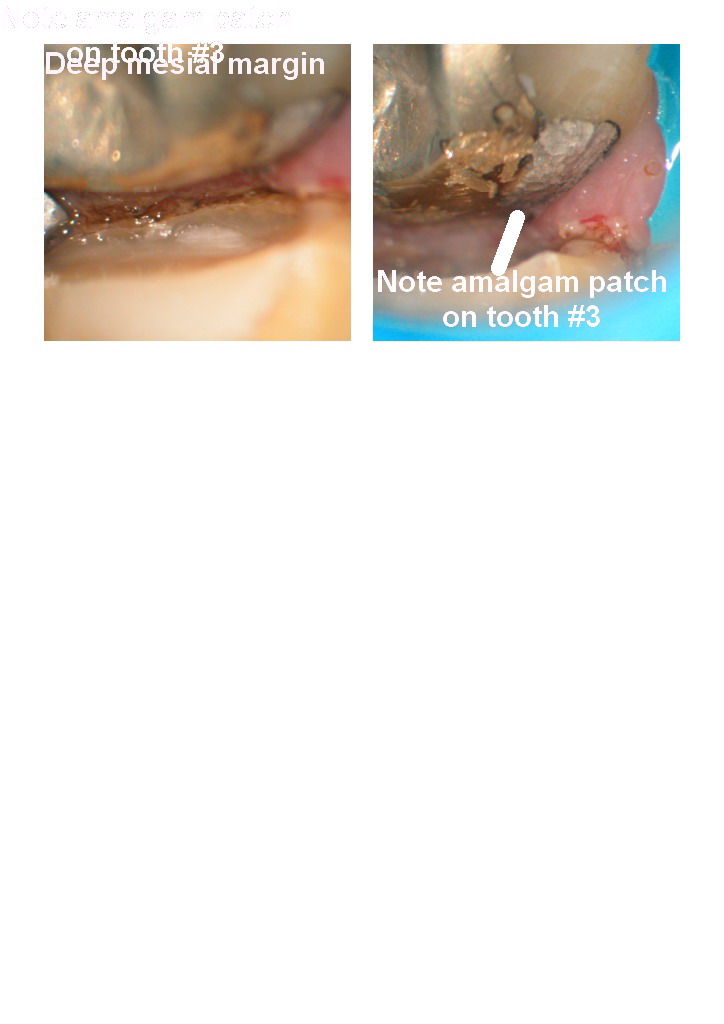
You know what , I showed him the Gold only on #3 with the DB amalgam under it (amazing that they can see that with the scope) and told him it should be replaced.
I never knew it was there til I prepped the #2 today, and on the Bitewing there was recurrent decay under the amalgam because of the food trap (see the opening pics of the open contact).
I showed the patient this and the very very deep amalgam which was blushing on the pulp.
Used the laser to sterilize and we will see how the tooth responds.
That is the beautyof the scope……..it is a great teaching tool for patients and parents to see what is happening.
Had a little 6 year old guy with a large DO on a primary maxillary left first molar. Mom and Dad came into the room to observe (and make sure that I did the right tooth) and were they ever astonished when they watch me on the screens in the operatory working on the little guy. They saw the decay, how close it was too the pulp and me doing it all without anesthetic.
PS Marks spoons were AWESOME…….thanks again buddy they are still sharp and boy oh boy did they work great and is that ever a eye opener for parents to watch you scooping soft decay out of their sons tooth …….
You cant show them that with 6.0 power loupes.
Thats the great power of the scope……documentation, ergonomics and finally education of staff and patients.
The practicum student we have for the next 3 weeks is in awe watching every thing we do.
Hope that helps and Kelly you really have a way of being positive……..DONT EVER LOSE THAT.
Glenn
PS THe Dental Clinics of N . AMerica should be out in the fall as I was the last guy to get his work in ……..what else is new…..spending too much time here.
140 references, 50+ pages and 12 clinical cases.
It wasnt a walk in the park.
Glenn
Dan MelkerSpectatorGlenn,
More and more I am intrigued by your pictures. Dave K. had told me he thought there was a restaint in Canada on how much a Dentist could do at any one time. True?
As a Periodontist that practices Rest. Dentistry. Meaning I will not do Perio surgery without a Rest. commitment if there is Rest. that is failing- I can tell you that if you find decay in a quadrant where there are old amalgams or patched up rest. usually all the rest. will have decay under them. Before the advent of core buildups we would simply cut down an old amalgam leaving a large portion and simply putting the crown over it. As I started reshaping teeth in 1975 I found that as I reshaped away a portion of an amalgam I would find decay almost all the time.
I usually do the rest. consult for my referring Dentists and use this same philsophy today. Replace a quadrant of old dentistry rather than tooth by tooth. So many times what I have said holds true. In many of your cases you do show one tooth with the adjacent tooth having a similar amalgam. Usually if done by the same Dentist in the same era usually the same will hold true.
Just telling you obervations over a 30 year period. Obviously that is not to say we down here in the south with the Tamps Bay Lightening replace all rest. I hope you get the jist of what I mean. Kelly observations are one that I have been wondering about and had asked Dave K.
Now, the more I look at your pictures the more I look at your pictures. They are truly amazing and are helping to put everything in perspective. I think I will be able to better understand what you are doing the more I see your pictures!
Thanks. Hope I did not bore you!
Danny
Glenn van AsSpectatorHI Danny……..you know what you are right. Part of the problem is that with the scope I find so much work to do that it is exhausting sometimes because I am booked 2-3 months in advance. There is no real restraint here but the dental plans wont pay for you to keep restoring all teeth.
One problem is that I am trying to switch my practice to a more dentistry on less patients with a quadrant philosophy type dentistry.
Good microscope centered practices such as Arturo Garcia and Dr. David Clark do this and I am trying to slowly follow their lead.
I totally agree with you on your findings and I could work 7 day weeks of 16 hour days and still be booked for 2-3 months doing this. I have that many patients in the practice (probably 4-5000).
With the scope and the documentation everything changes, its tiring sometimes seeing so much. I also have figured out a long time ago that the key to wowing others was pictures shot at 10x mag and above. People quickly realize that I am doing something different , both the patients and dental colleagues.
I appreciate your insights and will tell you that very recently I raised my fees ( a hard thing for me to do here in Socialized Canada – where we have the blue collar hardworking Calgary Flames- great series huh) and I am trying to get to the mentality of replacing all restorations or most of them.
Its coming Danny…….slowly but surely.
Take care my friend.
I will post some other stuff tonight………
Take care
Glenn
Dan MelkerSpectatorGlenn,
I think technology has got the best of you in a good way but initially it will be difficult. I believe when I first looked at your work I missed alot because really it takes time to truly understand where you are with the microscope.
As I have said all along you are a leader and I am truly beginning to understand where you are coming from. I like it alot! I am learning alot!
I think over time you will have to change your fees and time to the technology you have harnessed. Your documentation is extremely time consuming but really is necessary for Dentistry to go further. Raise your fees-you are well worth it. Start doing quadrants and see less patients-those that will pay for your quality services!
You have the gift-go with it!
Danny(Edited by Dan Melker at 4:35 pm on June 1, 2004)
-
AuthorPosts