
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Simple buccal laser restorations
- This topic is empty.
-
AuthorPosts
-
mickey franklSpectatorHi all
This is the first case I am presenting on the forum.
It is aimed at dentists out there who want to get a Erbium laser but are worried about the costI restored these 9 buccal attrition cavities (and 2 more occlusal small cavities) using my erbium laser to etch the dentine then placed composite fillings.The lower right second premolar cavity was subgingival and I did a gingivectomy too.
[img]https://www.laserdentistryforum.com/attachments/upload/buc cavities 11.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/buc cavities 22.JPG[/img]
All done in 90 mins generating an incom of £800(about 񘍔).
These could have obveously been restored without using any laser ,but the patient was very impressed with the Hi Tech experiance(no shot) and I do not think I would have charged that much without using a laser.Mickey
SwpmnSpectatorVery nice work, Mickey.
I like your blue retractors!!!!!
Al
Glenn van AsSpectatorNice stuff Mickey……how were you taking the photos and the erbium is great for these kinds of preps.
What settings did you use and for the soft tissue as well.
Great stuff…….nice to see others showing their cases regardless of how experienced you are .
Thanks again,
Glenn
ASISpectatorHi Mickey,
Good work with the laser. Not to rain on your first clinical post, but a connective tissue graft may be a more predictable long term solution to these ones though.
Andrew
Robert Gregg DDSSpectatorHi All–
Opinions please.
It is my understanding from reading the literature and talking with long time erbium users like Bryan Pope, that the erbium lased surface on dentin and enamel needs to be etched to remove the smear layer. Bryan said his 3 year post ops show microleakage that caused him a lot of concern…….
Comments?
Protocols?
Nice result Mickey.
Bob
Glenn van AsSpectatorTotally agree with that because the ablation products are present. I know this for a fact because if you etch the dentin after you prep it you will notice afterwards that the dentin takes on a different color postop (its not frosty anymore).
Now the erbium laser is supposed to open up the tubules so I was always wondering why the dentin changes color even if you etch only for 5 secs.
Use the etch on the tooth to remove the smear layer and on enamel make sure you use lower settings for the bevelliing to make less ablation products.
I will post a case in just a second.
Glenn
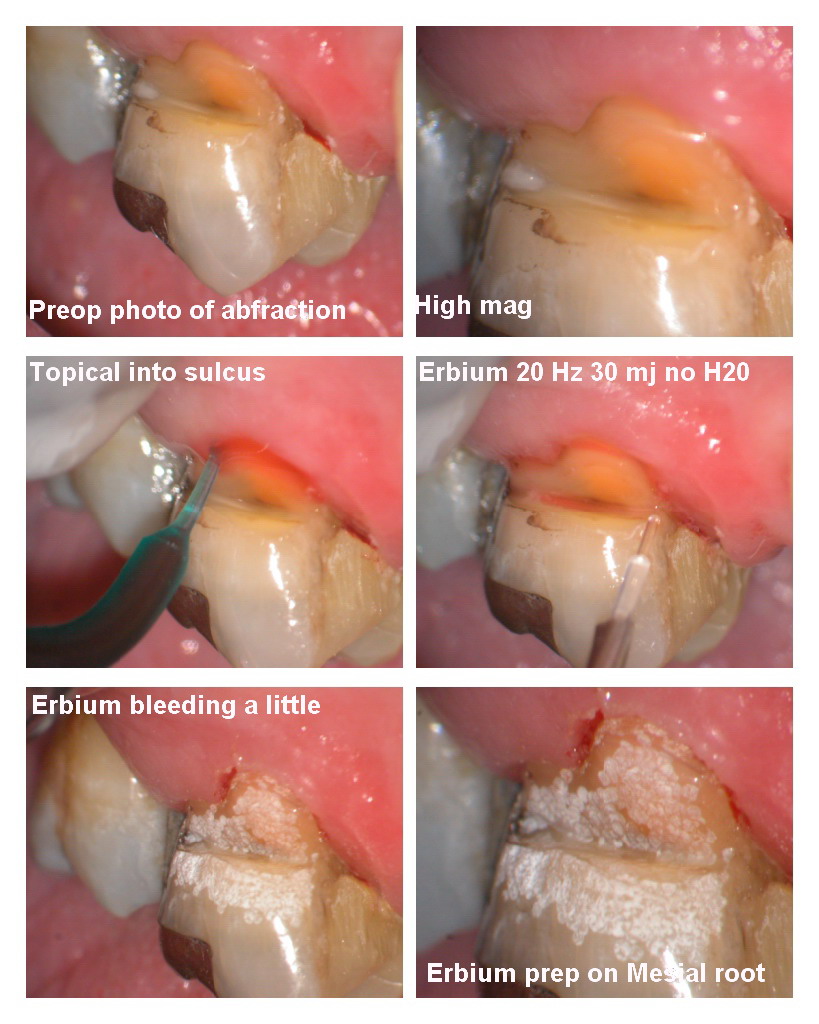
Glenn van AsSpectatorI am late for work but here is the case I did last Friday for a hands on group.
Abfractive lesion……older gentleman. No anesthetic except topical in pocket.
Used Erbium for soft tissue over mesial buccal root….
20Hz, 30 Mj no H20……..bleeding started a little.
Used Erbium for tooth at 30 Hz and 50-70 mj with water for the enamel I used the higher setting. Used a 400 micron tip for both soft and hard tissue.
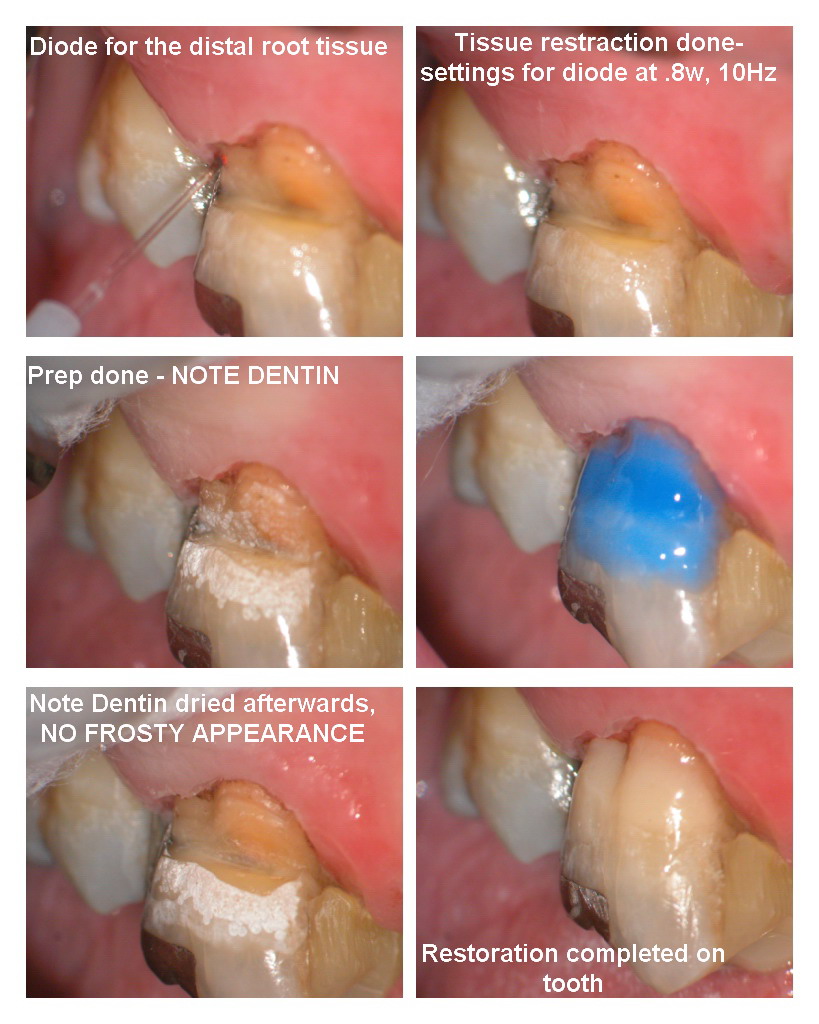
The diode was used on the distal root and to condition the mesial buccal root which was oozing and I didnt want a problem during the etch or bond.
It was an 810nm used at .8 w and 10Hz ….no anesthetic.
Patient felt it a tiny bit (3/10) but never felt erbium.
The dentin was frosty PRIOR to the etch , this is the key point to note.
Finished with Point 4 flowable (nice for class Vs as it is sticky and plasticky) and then polished.
Again note the difference in appearance of the dentin , it was dry both times but note how the frostiness disappears after the etch.
Glenn
AnonymousGuestQUOTEQuote: from Robert Gregg DDS on 10:02 am on Jan. 26, 2004
Hi All–Opinions please.
It is my understanding from reading the literature and talking with long time erbium users like Bryan Pope, that the erbium lased surface on dentin and enamel needs to be etched to remove the smear layer. Bryan said his 3 year post ops show microleakage that caused him a lot of concern…….
Comments?
Bob
Bob, if I remember correctly, Bryan was talking about the cervical of the proximal box where he was getting the leakage. I’d assume that maybe if the prep finished in enamel that the anhydrous byproducts, if not removed, would interfer with the bond just like on an occlusal. I think the solution is to mechanically scrape that area to make sure all the debris is removed. Also, for the majority of those, I now do Graeme M’s cocure technique and place GI there.
mickey franklSpectatorThanks for all the coments.
Glen photo with Olympus c4000 +photomed attachment,I needed Ron’s valuable help in uploading them because they were too big in size.settings for hard tissue 2w 60% air 30% water
soft tissue 1.5w 11/7
I used etch& bond all in one then composite.
Mickey
kellyjblodgettdmdSpectatorGreat posts to everyone on this thread. My two cents to add are these: uniformity of etch. We have all seen the SEMs that manufacturers provide to show how the dentin is supposedly free of a smear layer, and this may be true, but since your hand is constantly moving every pulse will have a different power density as it comes in contact with the tooth. One of the advantages of using 37% Phosphoric acid etch is that the quality of etching is uniform. I always etch after lasing, despite what my trainer (the sales person) tried to tell me.
Kelly
Glenn van AsSpectatorANother question Kelly is how do they prepare the surfacce of the dentin for the SEM process, does it involve any dilute acids that might rinse away the ablation materials.
I dont know the answer but clearly you can see at high mag the difference between the dentin pre and post etch. There is no question in my mind.
Glenn
AnonymousGuestBoard is slow (happens everytime Glenn become a world traveler) so I guess I’ll add some more buccal restorations. ER,CR:YSGG 1.0 watts 55/25 Fuji G- Bond and Gradia. Images with Revelation scope and G-5 camera.





SwpmnSpectatorAt this low energy setting, did you find that the white line effect at the incisal margin was minimized? Did you still hand plane the incisal margin? I’m doing some final enamel work at 30Hz with very low energy settings and finding that hand planing of the enamel margin provides little additional benefit.
How do you like the Gradia? I’ve been experimenting with Gradia and like the handling properties for posterior restorations. I don’t like the radiolucent properties of the anterior shades.
Al
AnonymousGuestfrom Swpmn on 9:14 pm on Jan. 20, 2005
QUOTEAt this low energy setting, did you find that the white line effect at the incisal margin was minimized?Al , I think it is minimized especially if you are well defocused
QUOTEDid you still hand plane the incisal margin?Always. Usually bevel with a small diamond. just read too much about leaving those ‘dreaded by-products of ablation’ behind and what they’ll do your bond
QUOTEI’m doing some final enamel work at 30Hz with very low energy settings and finding that hand planing of the enamel margin provides little additional benefit.Interesting. Not enough reason for me to buy hz adjustable laser, though 😉
QUOTEHow do you like the Gradia? I’ve been experimenting with Gradia and like the handling properties for posterior restorations.Like it alot but mainly use it in anterior as I still like tetric flow and ceram for posteriors
QUOTEI don’t like the radiolucent properties of the anterior shades.don’t think any composites should be radiolucent anymore, just makes it too difficult to diagnose around.
dkimmelSpectatorMickey great post!!! Nice use of an Er laser. Sure is easy to get a patient to do blocks of restorative when you don’t have to numb them.
Andrew, great eye and dead on.
Ron which light source are you using on the Global?? The pictures are getting better but not there yet…
30HZ at low mj really is nice. 50HZ is even nicer to finish enamel. Al is right.
Have you found with the scope that you are decreasing the Watts and staying more focused?
Al, I really like Girdia but you are right about it being translucent. I use the 0 shade first to add some opacity then layer. It can really look great. works great for those incisals of lower anteriors. -
AuthorPosts