
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › Simple frenectomies
- This topic is empty.
-
AuthorPosts
-
AnonymousGuestQUOTEQuote: from N8RV on 3:07 pm on May 25, 2004Quote:Quote: from andy on 10:25 pm on Mar. 11, 2004Please folks, I am not trying to be difficult. Periodontists are your friends. We want to help you provide excellent treatment for your patients.
As you know Glenn, I don’t try to put anyone down.
Andy
Don, please go back and do a search of all andy’s posts.
Andy has been most helpful and very good at offering suggestions. Janet wasn’t offended and I think everyone learned something.
I’d suggest in the future you heed your own words – “There are ways to present your pet peeves diplomatically and professionally, but that takes knowledge, patience, self-control and respect. ” So no more ‘for every colleague like you..’ statements please. Do those privately via email or phone.
Like has been said before- this isn’t DT
Thanks
dkimmelSpectatorDon,
Your off base on this one. I think Andy did the right thing. This is a forum to learn on. Not to just pat each other on the back and say how great a case looks.
As great as the net is , it is a very hard forum to communicate in. Posting a case takes a great deal of time. There is also a great deal of risk in posting. You put your work out there for all to see. It can be a great learning tool. Where else can you get such a varied source of insight. It can also be very humbling.
Responding to a post can also be tough. Often what we say can be read wrong. It is much easier to talk about a case with someone in person. Body language says so much. I can tell you your case looks like crap in person and you would laugh it up or punch me all depending on how I said it and what my body langauge was saying. Often it is tough to comment on someones work because we do not want to offend them . This is as wrong as unnecessarly critizing someones work.This forum is all about learning and sharing. I think we learn more from cases that could have been handled differently. We only see what we know and often we don’t know enough to see what we need to know.
Not posting cases it not only your loss but ours as well.
David
Andrew SatlinSpectatorDon,
If you choose not to present cases then you should blame your own insecurity and not me.
My suggestions were knowledgable and respectful. I did offer alternative treatment options. That was the whole point. I considered the patients complaint and the doctors clinical findings and offered what I believe to be ideal treatment. I did not just proclaim anything.
My understanding is that we present cases to discuss both our successes and our failures. That is how we learn and grow as professionals.
You however offer nothing but blind insults and inaccurate accusations. You have alot of nerve questioning my professionalism or my integrity. Many of the presenters can tell you from previous posts or those that know me personally that I am not self-righteous, boorish, rude or immature as you claim.
In the future, please keep you personal views about me and your advise to yourself.
Ron,
Thanks for your kind words.
Andy
Glenn van AsSpectatorHi guys……….. and gals.
You know what its hard to post stuff that you have done and feel proud of only to have people rip it to shreds. It sure makes it tough to post again.
I admire Janet for putting up her case in the beginning and I tell you what is weird…….
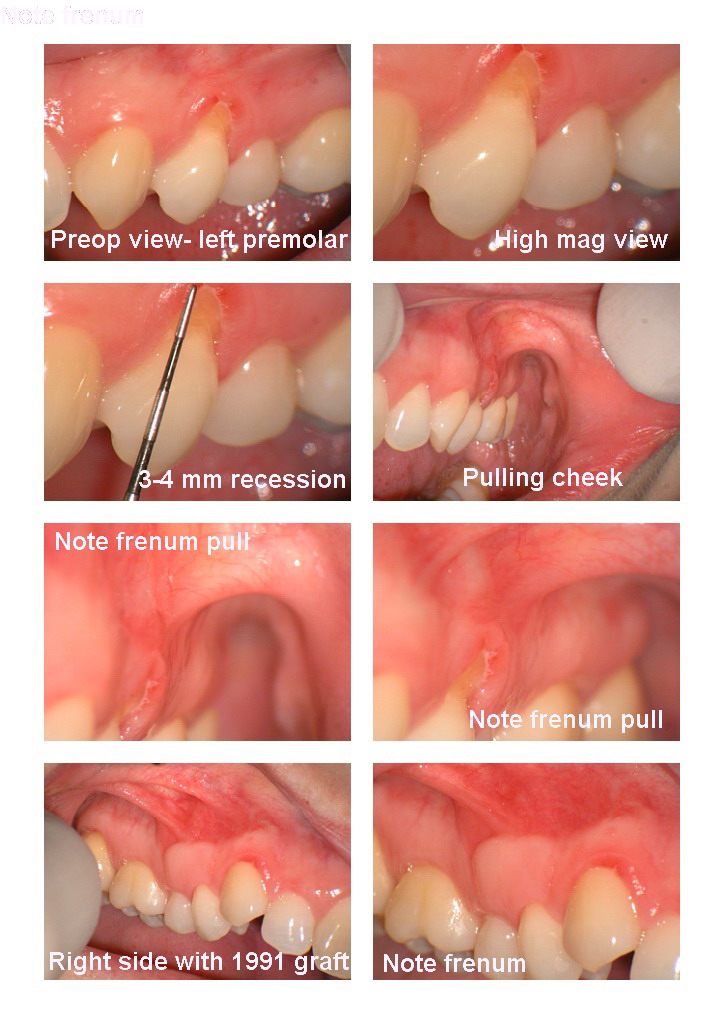
I saw this case today which was so funny because I photographed it.
THe patient has only 2 areas of recession in her mouth.
One is on the upper right first premolar and in 1991 it was treated with a graft in Switzerland and it had quite a bit of recession. It sure looks nice.
The other tooth is the upper left first premolar, now look at the frenum pull. Under the scope I could pull the cheek out and follow the fibers almost right to the premolar.
I am going to laser the frenum and in addition I am going to get her to the periodontist to do the graft. I am going to laser the tissue first and then do the graft at the periodontist.
I learned this from Andy and from Danny in their posts.
Don, thanks for coming on here. I will say that Andy was really very helpful right from the beginning when he came on this board. He really tried to be a big help and I was thrilled that a periodontist was trying to find out about lasers. His post on Janets case may have come out a little wrong , perhaps a little strong , but I have alot of respect for how he has helped me understand some things, as Danny has helped me with Biologic principles (maybe in a little different fashion…..GRIN)
Now Danny has come on board and I have noticed that recently he has really tried in the graft thread to help us all out and not fly of the handle because of something someone said or did.
Kudos to him for that, and having never met Danny I think that he is incredibly knowledgeable about perio and probably a very good periodontist. He shocked me with his first few posts here and on DT about things that I was doing but he is seemingly trying to make good.
Dont let the differences in opinion stop you from coming here Don, as Ron Schalter has put up a great site here that is of incredible value. Peruse through some of the old posts and even see all the mistakes I made and still do make!!
I have learned from alot here and think that you will too and dont be scared to post here. I want to thank you for your kind words, its a win win situation when you post here as others learn and you learn a little about yourself ( and how you deal with constructive criticism) and improve as a dentist.
All the best and here is the case.
Glenn
Dan MelkerSpectatorJanet,
As I have been in Andy’s shoes, it is not fun. With that said and knowing that neither Andy nor myself have been diplomatic at times keep posting. We both love Perio and may not know how to get points across at times with proper diplomacy.
I have read quite a few posts and I would like to share my observations:
1. Let’s look at this case if it were done with a scalpel not a laser.
2. A young patient with problems on #3, 4, 5, 12, 13, and possibly # 29 from the pictures.
3. There is very little frenun involvement on those teeth that were not treated with frenectomies.
4. Occlusion-could play a part and should be checked. Just a clinical statement of fact. Between 1975- 1982 I did almost 1500 grafts and never once touched or checked the occlusion of the tooth. My lack of understanding occlusion, yet a followup of approximately 1000 grafts up to the present shows almost a 100% success rate. That is simply a statement of a clinical fact. Around 1982 I started to learn about occlusion and a healthier respect for it now.
4. Genetics-not the patients parents but palatal tissue. Palatal tissue is dense thick connective tissue and when it replaces the tissue present where the mucogingival problem is, it brings those characteristics with it. That is the reason for such success with attached tissue procedures.
5. In my opinion Andy is right. On DT under recession and grafting by D. Kimmel under perio section there are several Subepithelial connective grafts shown. These type of grafts would have been well suited for this young patient. It is not to late. One case 0f #6 shows a SECTG. placed on top of a classV restoration. As I have said on other threads SECTG’s have been around since 1986 approx. I have been doing them with success since 1989. Early years I had considerable failures. Now I have almost 100% success long term with documentation to prove it. Lately I have modified tech. and should being running 100% all the time. I am saying this not to say look how good I am but look how great the procedure is!
5 Finally,connective grafts do two major things:
A. prevent spread of bacteria to underlying osseous beause of avascular tissue
B. because tissue is dense connective tissue it prevents recession from toothbrushing(trauma)
Janet , you should keep posting. People like myself and Andy just need to respect what you are trying to accomplish and speak in those terms.
Thanks,
Danny
As always sorry for any misspelling(Edited by Dan Melker at 6:58 am on May 26, 2004)
(Edited by Dan Melker at 7:02 am on May 26, 2004)
N8RVSpectatorThe last thing I want to be accused of is being a “hit and run”, so I’ll at least reply to the lashing I’ve been given.
I’ll be the first to admit that, even with the most well thought-out comments, things can be misunderstood. As was rightly pointed out, written communication is lacking at best. However, were I the recipient of Andy’s comments, I’d be as far gone from this forum as I could get!
Andy (and all), if my criticism of your response to Janet was too harsh, my apologies. It is a reflection of the other rude and impolite posts that have caught my attention where I’ve started a reply and hit DELETE. You became the lucky target of my frustration, I suppose.
Another thing that I must admit is that I responded without reading all the posts on this topic. I didn’t realize that there was more than one page, so the continued discussion, including Andy admitting that, given more information, he would’ve accepted the treatment, was unknown to me. Had I read both pages, I likely would’ve dismissed Andy’s initial comments as being merely emotional.
All I’m saying is, play nicely. When people are rude and inconsiderate it demeans the profession. Because we are communicating with a measure of anonimity, we tend to be more abrasive and cocky than if we were facing the risk of getting socked in the mouth.
I won’t beat a dead horse. Again, my apologies for ruffling anyone’s feathers with my plea for some civility and professionalism. I’ll go back to lurking and learning. If I have any questions, I’ll contact the poster privately. I don’t have a problem with that.
Have a good day all.
(Edited by N8RV at 9:29 am on May 26, 2004)
AnonymousGuestQUOTEQuote: from N8RV on 9:23 am on May 26, 2004
I’ll go back to lurking and learning. If I have any questions, I’ll contact the poster privately. I don’t have a problem with that.Have a good day all.
(Edited by N8RV at 9:29 am on May 26, 2004)
Don’t go back to just lurking. Ask the questions on the forum because I’m sure many are asking the same thing.
kellyjblodgettdmdSpectatorI thought that the purpose of this forum was to help eachother provide better care. Certainly, this requires that when we post we be ready for advice on how to do it better, or at least listen to different approaches to care. It requires that we have “thick skin”, and more importantly, that we understand that we don’t have all the answers, or always know how to provide the ideal treatment.
I am thankful for the periodontists that are willing to be critical (hopefully it’s constructively worded) so that we might learn how to better serve our patients. I hope that Janet and N8RV will feel comfortable to share their cases. I have found that I learn far more when people challenge my thinking than when they pat me on the back.
Kelly
ASISpectatorHi All,
No question about what Kelly stated. I have learned more from making mistakes than from not. But, somedays are better lived if a little less learning took place.
Andrew
kellyjblodgettdmdSpectatorAmen, Andrew.
Kelly
-
AuthorPosts