
Forums › Erbium Lasers › General Erbium Discussion › This is FUN.
- This topic is empty.
-
AuthorPosts
-
Graeme MilicichSpectatorBeen playing around with the C6 tips more and more. They have an interesting “footprint” that changes as you defocus the beam. It goes from a focused zone, and as you move away from the surface, the main energy distribution becomes like a doughnut. This helps prevent central overheating and whitespots. Move out a bit further and the beam diverges quite rapidly. This effect is beneficial if you want a wide footprint for certain effects. Here is a soft tissue application of the C6 tip utilizing its defocused, wide footprint.
This case is only simple stuff, but it helps make a difference. Had this patient in today with subgingival caries. A real “potty mouth.” Can’t get him to clean his teeth any better than this!!! Been beating my head against that wall for 10 years. He won’t make the connection between cleaning his teeth properly, and avoiding making regular contributions to my retirement fund!!
The buccal gingival tissue was very thick and rolled and covered most of the lesion. So I used a C6 tip at 1.5W 7%W 11%A in a defocused mode to utilize the wide footprint of the C6 defocused beam to contour the tissue for access.
It was incredibly effective in ablating away the full width of the tissue (about 1.2mm wide) without creating the potholes in tissue that the G6 tip tends to create because of its more focused beam. Normally, I would have used a 750 micron tip and still had a bit of difficulty dealing with the width of tissue in one sweep.
Once the height was established, I reduced the power to 0.75W 7%W 11%A and did an internal reverse bevel gingivectomy with a focused C6 tip. This thinned the thickness of the tissue and gave better access without reducing the height any further. It will also allow the tissue to collapse back onto the tooth and create a thinner gingival architecture, which hopefully will reduce plaque accumulation in this site. (one can only hope!!)
IMHO, there was sufficient attached gingival to make this treatment option viable. Repositioned sliding flaps etc would not be indicated in this mouth!!!! Cost being the major player, plus potential healing issues due to the poor oral hygiene. Eating into the attached gingiva might not be the perfect periodontal approach, but sometimes our options are limited by other patient factors.
—

Initial contouring. Cord and astringident used to establish a dry field (crevicular exudate more than bleeding)
Composite placed
Cord removed and composite polished (Optibond and Gradia Direct)If I had tried to do this with a G6 tip, the energy footprint would have been narrower and it would not have covered the entire width of the gingival tissue. It would have still got the job done, but would have taken more time and would have not been as smooth. This doesn’t look very wide on the crest in the photos because I have removed about 3/4mm of width with the internal bevel gingivectomy. I don’t think I could have done this with a scalpel or electrosurgery. It only took 2 minutes to establish a clear operating field for this restoration.
There was an intersting string recently where a keen user commented that laser dentists were “better.” I don’t think that is what was really meant in the heat of the enthusiasm. I think this little case is what was being alluded to. The laser can let you personally do “better dentistry” compared to what you would have personally acheived without having it at your disposal.
Every day I do little things without thinking about it, and then realize how much I have integrated the laser into my treatment protocols without realizing just how dependant on it I have become.
If you haven’t got any of the new C6 tips, get one and take it for a spin.
Cheers(Edited by Graeme Milicich at 5:27 pm on Oct. 20, 2004)
N8RVSpectatorGood post, Graeme. A good example of “everyday dentistry” that may not fall cleanly into a chapter of a periodontics textbook.
So many times, I’ll see posts by well-meaning and talented specialists outlining some amazing, exotic treatment that just doesn’t fit my typical patient’s needs. Often, time or financial constraints will prevent us from providing that optimal treatment.
I hope you can snap a quick picture or two a couple months down the road as a followup to demonstrate the healing. I keep meaning to do that, but forget which patients on which I’ve done these types of gingivoplasties!
— Don
(Edited by N8RV at 10:04 am on Oct. 20, 2004)
AnonymousGuestThanks for the info on the C6, Graeme.
Just curious, why no GI for the restoration?
marc andre gagnonSpectatorGood post,
an excellent case of “everyday dentistry” that we can do with laser .
The kind of treatment that laser dentistry can offer to patients .
I hope you can snap pictures to demonstrate the healing.
Thanks to share with us
Graeme MilicichSpectatorQUOTEQuote: from Ron Schalter DDS on 1:19 am on Oct. 21, 2004
Thanks for the info on the C6, Graeme.
Just curious, why no GI for the restoration?I was planning on doing a Fuji lX, but my assistant already had all teh composite stuff out and was ready to go, so I just went with the flow
SwpmnSpectatorGraeme:
Can you post a photo of the C6 tip?
Is it 6mm in length? Is it a tapered or parallel tip? What are the width dimensions in microns at the proximal and distal ends?
Thanks,
Al
whitertthSpectatorGraeme,
Great case…I have used the c-6 extensivley…It is a great tip for thinning out papillas in Dialntin Hyperplasia cases or mouth breathers. U can actualy plane the papilla right down with a few passes without the pothole affect that Graeme describes that U would get with a G-6 or T-4…Nice stuff graeme..
ASISpectatorHi Graeme & Guys,
As Glenn had stated a number of times before, lasers make doing difficult procedures in dentistry easier.
Just like in Graeme’s case, if you can recontour the tissue to gain access and proper isolation, how can one not do better. With the use of laser to allow the treatment to be handled better, and not to mention the benefits to the patient, why would one not continue to do so.
We are all creatures of habits. We are what we do.
Thanks for the case, Graeme.
Regards,
Andrew
2thlaserSpectator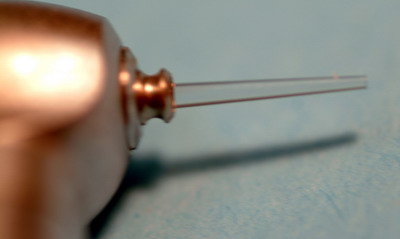
Allen,
Here is a pic of the C-6. It’s 9mm long 1200microns at the distal end tapering to 600 microns at the tip. It’s energy pattern is more concentric and flat….
I am in Germany, and will upload a graphic pic later cause my Lisa is begging to go out to dinner! It will show the energy pattern. This is truly a GREAT tip. AND we are working on a 6 and 4 mm version of this which should really be cool.Mark
Graeme MilicichSpectatorAl
Further to Mark’s post
These tips have quite a steep drop in energy compared to the G6 tips so need to be operated at a slightly higher power setting compared to the G6 tips to get a similar ablation rate.The energy footprint is smooth compared to the G6, which is hot in the middle. This is why you can use it so effectively for surface ablation without creating the pothole look on soft tissue.
I wish I had taken a photo of the ablated ridge before I did the reverse bevel gingivectomy so you could see the difference.
Cheers
Robert Gregg DDSSpectatorAny suggestions as to the etiology of the lesion?
Thanks,
Bob
Graeme MilicichSpectatorBob
are you asking about the carious lesion or the soft tissue?
Lesion = potty mouth.
Soft tissue = chronic inflammation and gingival crest fibrosis associated with long standing poor oral hygiene. This tissue thickening was creating an even better plaque trap which lead to the cervical caries.Recontouring the tissue had two goals. Firstly to get me access to the lesion, and secondly to modify the gingival contour to help reduce plaque accumulation
Cheers
SwpmnSpectatorThank you Mark for the photo/specs and to Graeme for further clarification on the C6 tip.
Al
-
AuthorPosts