
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Yet Another Crown Prep….Part II!
- This topic is empty.
-
AuthorPosts
-
SwpmnSpectator80 yo female presents with lost DO amalgam and fractured lingual cusp on mandibular right second premolar(#29):
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa090204-1.JPG[/img]
Profound chemical anesthesia was obtained via 4% articaine 1:100K epinephrine placed at the mental foramen. Tooth was then grossly reduced with a HOYA ConBio DELight 2940nm Er:YAG using a 30 degree 600 micron tip and console setting of 25Hz 300 mJoules. Copious distilled water irrigation was applied via the laser tip. Gross reduction took me 15 minutes.
The Er:YAG console setting was then adjusted to 30Hz 85 mJoules and utilized to smooth the prepared tooth(5 additional minutes). At no time was a conventional high speed dental handpiece used on the tooth. A HOYA ConBio DioDent 810nm diode laser was used with an activated 300 micron fiber on a Continuous Wave 1.0 Watt setting to retract gingival tissue around the preparation margins. Additional chemical anesthesia was not necessary for retraction of lingual tissue or for hemostasis:


Impression placed using standard techniques and die returned from laboratory technician(just for entertainment I did not tell him this was an erbium laser prep):
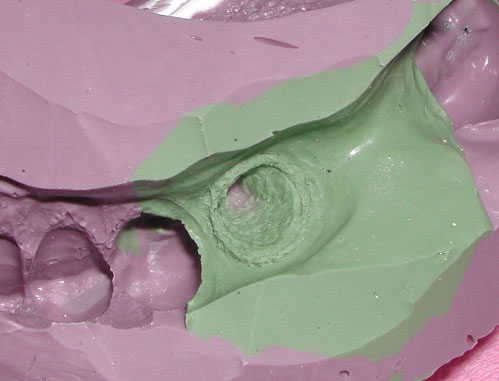
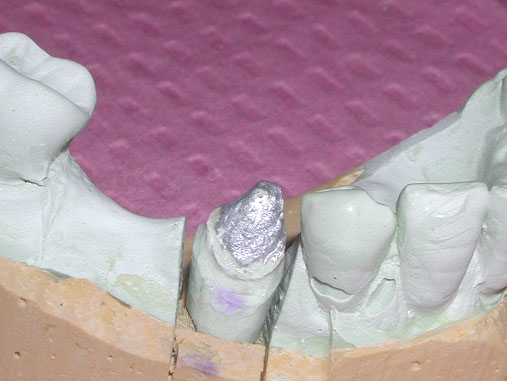
Photo of preparation on crown seat day:

Images of crown on seat day:


Please feel free to comment and provide constructive criticism of the case so that we may all learn. There are an infinite number of ways to criticize this case and I make no claims that my approach reveals any benefit over conventional preparation techniques. In fact, it takes more time and appears to result in preparations which are not as smooth as teeth prepared with diamond burs in high speed handpieces. The purpose of my post is two-fold:
1) To re-confirm the findings of Colonna and others that there are alternative tools available to prepare teeth for indirect restorations. Like many others, I scoffed at Colonna’s original presentation.
2) To demonstrate that by observing the evolution of Colonna’s original technique it is possible for other practitioners to improve on their own technique. For example, here is my original erbium laser crown prep from November 2002:

Al
Glenn van AsSpectatorNeat neat neat Allen……….
I know Mark is cutting down the enamel at the DEJ and breaking off the enamel with an instrument. How did you reduce the tooth structure.
I like the final result it sure looks nice in my opinion and there is no question that the prep is much smoother than the first one you tried.
Amazing to see the final smoothness of the margin photographically. Do you think that the 30 Hz allows for a smoother bevel than a 20 Hz setting. I am just pondering what you have found.
Do you find that visibility and access is best with the Delight tips compared to the contra angle and why the 30 degree compared to the 80 degree.
Interesting as well to not that the unit you are using is capable of 7.5 watts which is what you used. Thats cooking man!!
I think that is really great. I have never done a crown prep but I think your case was the right one to do it on. You gotta have patience to do this though, and I for one admire your dedication to the completion of the task with the laser.
I will say that the best picture that you have is the one at the end of the post!!…..you would hardly recognize me now with all the weight I have lost jogging!!. Time for a new picture at the ALD this year. Maybe we can get that hygienist from Oregon to pose with us!!
GRIN
All the best
Glenn
whitertthSpectatorAl,
Nice prep, I have done a bunch myself and what I teach in my courses is how to be able to do this in case a patient seeks u out for pure laser dentistry and dont want drills…..Some have already done that here, and as patient education about the potential of lasers increase, we will see more people asking for it…I still think for me it isnt time appropriate….How long did it take start to finish? Great Job and nice case….
2thlaserSpectatorNice Allen,
The one thing I notice is how well you use the laser compared to the “early” years. Showing a great proficiency in all areas of laser useage. This is a case that shows you can prepare a tooth without the use of a drill, AND, how easy it can really be. How was the fit of the margins with your explorer? Just curious. Great tooth to prep as well. I bet it didn’t take too long either. Was there a reason (not being critical, just asking for curious reasons) you used chemical anesthesia vs. laser anesthesia?Nice….
Mark
Glenn van AsSpectatorMark I dont know if you have a diode from Biolase but it is darn tough to trough without anesthetic with the diode.
Oh sure it can be done with settings like .8w at 10 Hz but its slow. Now the patient is 80 and this helps because often there is less sensitivity.
I for one am not a big fan of sticking the erbium into the pocket to trough unless you use large loupes or a scope. You can nick your margin easily, so make sure your settings if you are erbium troughing is less.
If you keep your margins high and dry no problem.
Hey Mark, we missed you, try to check in with some of your great insight more often. I for one miss it.
Glenn
SwpmnSpectatorGlenn:
For the gross reduction, I simply turned the tip perpendicular to the occlusal and “chopped off the top”. The tip was then turned parallel to the axial walls to strip the enamel at the DEJ – similar to stuff I’ve seen Colonna and Ben Ong present. Tricky to develop an axial taper compared to bur usage. You can see where I overtapered in some areas and underprepared the lingual axial wall.
The 30 degree DELight tip was used because there is less energy loss along this tip compared to the 80 degree tip – therefore increasing the speed of gross reduction. An awful lot of energy was applied to this tooth yet the patient experienced no symptoms of reversible pulpitis. The console energy settings reported are only marginally useful due to wide variations in erbiums. Ideally we should measure energy output at the tip. It is possible that the 30Hz setting gave me an advantage in smoothing the margins, however, I have seen Colonna and Schalter obtain smooth margins using 20Hz.
Ron K.:
I carefully timed the preparation at 20 minutes. 15 minutes for gross reduction, 5 minutes to smooth prep and refine margins. Obviously that is a lot of time for a premolar crown prep. What I was trying to do here is to see if I could obtain an acceptably smooth prep without using a diamond bur – like I have observed Colonna present in his revised technique. Another goal was to prepare the margins without inducing the soft tissue trauma which you can see was created during my first crown prep.
Mark:
Clinically, the crown appeared to have excellent marginal adaptation. Ideally, for case presentation purposes I should have exposed a bitewing radiograph. Since the crown seated perfectly with only minor occlusal adjustment, I saw no reason to justify the radiograph.
Regarding chemical anesthesia, it is simply a personal preference and allowed me to focus on developing an acceptably smooth preparation. It’s entirely plausible that this tooth could have been prepared without chemical anesthesia. We do not place chemical anesthesia for the sole purpose of using the diode for tissue retraction. The diode laser has allowed us to reduce our application of chemical anesthesia on lingual/palatal soft tissues and greatly reduce our usage of lidocaine with 1:50K epinephrine for purposes of hemostasis.
Al
2thlaserSpectatorAl,
In one word….AWESOME! Nice. I notice that the fit of laser prepared crowns are really really nice. I mean really nice. That’s why I asked what you evaluated clinically.Glenn, Sorry I am not on as much, just too busy for my own good. Lot’s happening in my personal and professional life, and am trying to find that “balance” we all look for.
Miss all you greatly!
Mark
ELLIOT ROGOFFSpectatorThe work shown in this post is very admirable and yoou should be commended for your fortitude. I have read many posts on this technique by Mark and Co. and all are fine. I have a question for the group (being a new laser use and a novice) why in the world would we want to take 15-20 minutes to do an okay job with the laser when we ALL can do this with a handpiece in 5. If the answer is “Because we can” that’s okay but I still think that dentistry should be done to the best of our abilities in the shortest time possible. The laser is great to use and I am enjoying all the possbilities but for crown preps I have my doubts. This should stir things up. Elliot
arrowsmithSpectatorElliot,
You are absolutely correct in your questioning the validity of such a procedure. I can tell you I still way prefer the handpiece over the laser for crown preps. The reasons why I have chosen to do a laser crown prep in the past was for the following;
* The patient wanted it done.
* I simply was itching to do it . . . just because I could.
* Potentially less trauma to the tooth, including less heat, no microfractures, no smear layer, and less post-op sensitivity
* Mark does ’em in 6-7 minutes!!! Now I really gotta try it!!
* I paid โK for this thing and I want to get the most out of it . . . . you really find out how the laser works when doing a crown prep with it.Another great potential for laser ASSISTED crown preps, where the prep is done conventionally and then the laser removes the smear layer or refines it ever so slightly.
Thank you for stirring things up!!
aaroN
SwpmnSpectatorQUOTEI have a question for the group (being a new laser use and a novice) why in the world would we want to take 15-20 minutes to do an okay job with the laser when we ALL can do this with a handpiece in 5.Elliot:
Best question anyone has proposed. Here is why I did it:
To demonstrate the evolution of the laser crown prep technique and prepare myself for the FUTURE
My personal assessment is that we are currently in an early, primitive and pioneering stage regarding the usage of alternative tools to prepare teeth for restorations. As I’m sure you are already aware, patients clearly prefer the audible advantages and the lack of vibration created by the erbium lasers. In the future, it may be possible to develop better lasers or other tools which can reduce teeth in a timely fashion.
This is not a technique which I advocate on a routine basis. In fact, over the past two years I’ve probably done five erbium laser crown preps and this was the first one where I did not use a dental handpiece to smooth the prep. The purpose of the case presentation was simply to show that an average general practitioner can improve on an alternative technique via listening and reading.
You aren’t stirring up the thread, what I’ve found over the last three plus years is that we learn the most by disagreeing. Pats on the back do nothing to advance the science of dentistry.
Al
Glenn van AsSpectatorAw shoot Allen , now I will have to criticize you instead of patting you on the back.
In all honesty I have never done a crown prep at all. I am not patient enough.
I also think personally that looking through the scope it is too rough for me and I prefer the control I achieve with burs but that is totally a personal opinion.
I agree constructive criticism and asking questions in the tone that Elliot asked is great for trying to grow as a practitioner.
The road to success is paved on failure…………
I am off to finish my lecture but neat case.
Glenn
ELLIOT ROGOFFSpectatorThanks Aaron and Al for responding to my question. Now that I have heard from you I can’t wait to do my first crown prep with my Erbium. I will set aside enough time just in case my hand touches the dreaded drill and I need to touch some things up. You guys are great and I can’t wait to meet all of you in New Orleans. Elliot
-
AuthorPosts