
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorI have 2 suggestions…….
1. If you want point and shoot many of the experts are getting a Canon G3 and adapting it with a macro lens and ring flash from someone like Photo med.
Tarun at Dental Town has alot of posts on how to do this under the digital photography section
2. If you want better pics quality wise, a little heavier camera and enjoy shooting pics outside of dentistry you may want to use what Mark Colonna has and get a Fuji S2 with a 105mm lens (either Nikon or sigma) and the Sb 29 ringflash from Nikon.
It will cost you more but you can take off the lenses and shoot family stuff with other lenses. Do you have any other lenses at present and what is your camera knowledge and how much do you want to do with your camera……..
Only at the office and simple stuff……..look at the Canon G3
Take other stuff with a variety of lenses then look at the Fuji S2 which is more expensive……
Glenn
Glenn van AsSpectatorBy the way that protector is called the INTERGUARD by Ultradent and is pretty thick so sometimes I have to pop it out and take a sectional matrix to get a nice contact.
The metal matrix seems to help cut faster in the box because of reflection from the metal.
Glenn
whitertthSpectatorThanks for the tip…I actually did that on an anterior tooth today…my card reader crapped out so i couldnt post it yet….I restored the tooth with kerrs point 4…seems like it does a nice job…i have restored primary teeth in the past with compoglass because of the FL. but i think it may be a crock and it dosent polish so well so i have gotten away from it …..
whitertthSpectatoris there a problem with using regular toffelmyre matrix bands as protectors?
whitertthSpectatori use a photomed epson camera …I thinks it s a very good intermediate camera…but u guys r the best judjes…. the problem is photomed constantly changes their packages and they dont even sell mine anymore….
they will support it fi need help but they are also not cheap to buy from…If u want to buy or learn more i would call Andy Thompson at Norman camera(http://www.normancamera.com) . tell him I told u to call…he is very knowledgeable, has dental packages and dosent rip u off… He supplies the camera now for pac live…. Good luck!
AnonymousSpectatorHere’s another er,cr:YSGG .75W 7 air ,no h2o, EMLA topical.
Preop picture

Immediately after TX

24 hours later

(dark spots in 24 hour are artifact,n0 charring present)No pain or discomfort at 24 hour mark.
Will post again in 1 week. Its interesting that this pt had lesion area of # 8 about 3 weeks ago- no recurrence there but rather the new spot.
Glenn van AsSpectatorI agree Ron look at Norman Camera. They were there even before they started with the dental market.
Glenn
Glenn van AsSpectatorgreat question…….there isnt a problm its just that sometimes when the contact isnt broken they are darn tough to get in
The interquards are quite firm and easier to get through.
Being thick its tough to get a good contact with the interquards from Ultradent.
Just a thought……….
Good stuff Ron and nice pics
Glenn
AnonymousSpectatorWhat about mirrors ?
What kind? for occlussals , buccals, linguals,etc.
From where?
Do most kits include these?
I have the Morita retractors, nice but seem a little fragile.
PatricioSpectatorHi group,
As a novice your pics are a great help as they pretty much confirm what I have been doing. A confidence builder. I have found I like to cean up with a round bur and then finish with the laser to a hard smooth surface. I do notice sometimes at that point there can be stained dentin left at the base especially with some more vertical decay uncovered by the diagnodent. Are you guys removing that as well? In the olden days I would have cut it out but thinking concervatively I have been leaving it when I am convinced it is firm.
Pat
Glenn van AsSpectatorHi Ron and best wishes for a happy new year. Man your forum is taking off……kudos to you.
Hey I have a variety of big mirrors and basically I use the occlusal mirrors either large or small. If you do ortho you need the buccal ones but for photography I just have the ones from Washington Scientific or Photomeds and they work great.
I just think you want to avoid having the distraction of lower teeth staring you in the face when you are photographing the maxilla. Now with the scope , I just bump up the mag and it all disappears if there is a distraction from another area.
Photography through the scope is a breeze.
Glenn
Glenn van AsSpectatorI remove everything I can, hardly ever leave anything but I am the first to say that the laser can make it very difficult to tell what is decay and what isnt.
The water acts to rehydrate the decay and the color goes from obvious orange to dentin yellow. The only thing that helps me is the texture at high mag is much more obvious of decay. If in doubt I take a spoon…….(Hey Mark where are those spoons!!!) and check.
Caries detector give you false positives on the enamel and makes it tough to remove the color from the etched enamel.
I love small round burs for large soft areas and in addition for decay tracking laterally. Patricio you are far from a rookie here and the great thing about this forum is the general level of comraderie and interest in learning.
There is a learning curve to using the laser but seeing the cases posted here sure helps shorten that.
After 3 years of working with the laser and a scope, I have tried alot of things but people here constantly push the envelope and make it more interesting each day to practice as the cases always come outside of the box.
Keep it up, and I will post another simple case in a minute.
Glenn
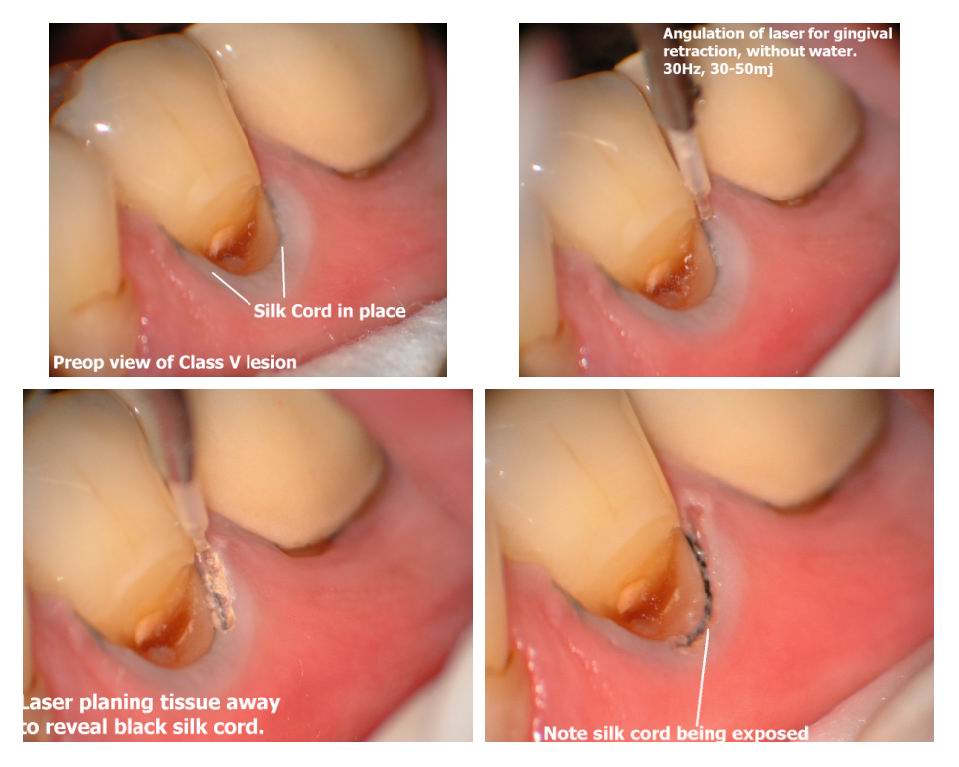
Glenn van AsSpectatorHi folks: Here is a Class V abfractive lesion and boy these are a joy to do with any erbium.
You can remove tissue on the labial without anesthetic with water off (air if needed on the Biolase) and if you get one tip out of this , its to buy some silk cord (silk thread) and place it in the crevice prior to removing the tissue and it acts to help you in two ways.
It protects the deeper structures that are beyond 1mm like pockets, bone and especially cementum.
In addition it provides a visual marker for you to lase to and doesnt really get too damaged by the laser.
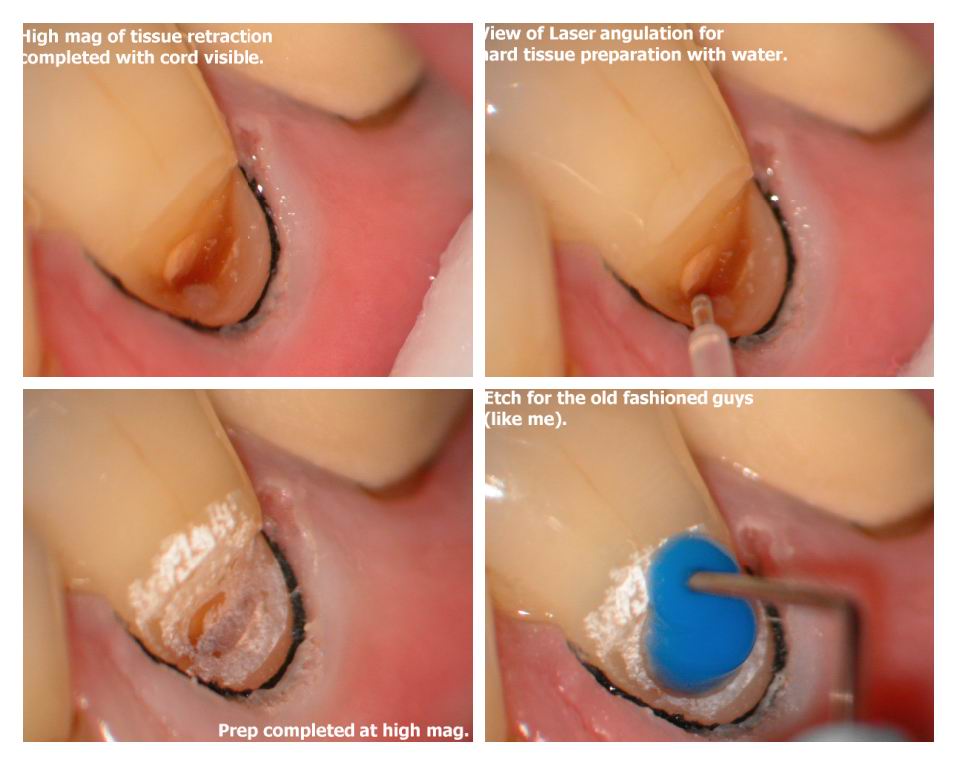
The composite was a little light. Use water with hard tissue removal and a little higher settings.
Soft tissue was 30 Hz and 30-50mj (.9-1.5 watts) with no water at all (you can use air if you want)
Hard tissue was 30Hz and 50-70 mj (1.5-2.1 watts) with water starting defocussed if you want.
I will post a case where I didnt use cord, didnt take caution with the cementum and show you my mistakes in a sec.
Glenn
Please tell me if these pics help you at all.
By the way……..no anesthetic with this one.

Glenn van AsSpectatorThe photos are in 4 per page so read them as follows
A B E F I J
C D G H K LSorry for the confusion but its the way the forum reads the pages.
I will have to stick to one page………
Glenn
AnonymousSpectatorQUOTEQuote: from Glenn van As on 3:02 pm on Dec. 29, 2002The water acts to rehydrate the decay and the color goes from obvious orange to dentin yellow.
GlennI’ve found that many times I think I’ve got everything and then etch (see previous post regarding difference in surface of etched vs. laser etch teeth) ) and dry only to find the discoloration. At this point I again pick up the slow speed, remove remaining decay, re-lase (word?) the area and finish. I’m also using Graemes co-cure technique more and more – figure the glass ionomer is a good thing to have there if any doubt.
-
AuthorPosts