
Forum Replies Created
-
AuthorPosts
-
kellyjblodgettdmdSpectatorMark: Thanks for the great visual! The cross-sectioned tooth really helps me visualize the process. Keep up the great work.
Kelly
2thlaserSpectatorThanks Kelly, I just get these questions all the time when I am speaking, and I thought, I needed a visual to show everyone. When I show this in a “hands on” format, I ALWAYS get the, “now I got it!!” exclamation about a day or so when they get back to their offices. SO, that being said, I thought this might be a help in visualizing the way it seems to work the fastest for those who seem to be having problems with what I consider the most easiest of preps…ok Class V’s are probably easier…but you get my drift!
Thanks,
Mark
Robert GreggParticipantThanks to Ron and Glenn, I’m making my first attempt at taking, editing, and posting my first digital photos from my recently acquired Nikon 4500.
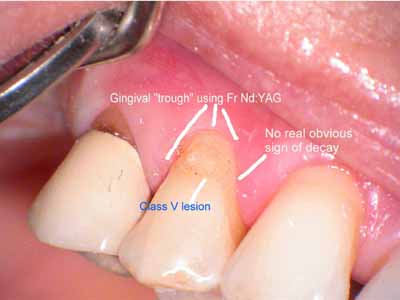
Used 4.0 Watts and 20 Hz, 100 usec PD to trough the gingiva from distal to mesial and accross the facial to expose the margin of the tooth, obtain hemostasis, and control the egress of gingival sulcular fluides.

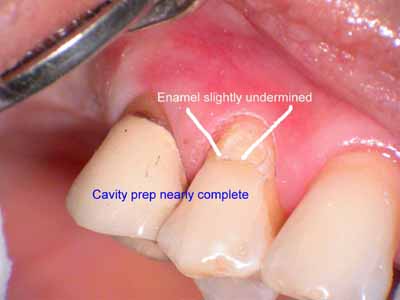
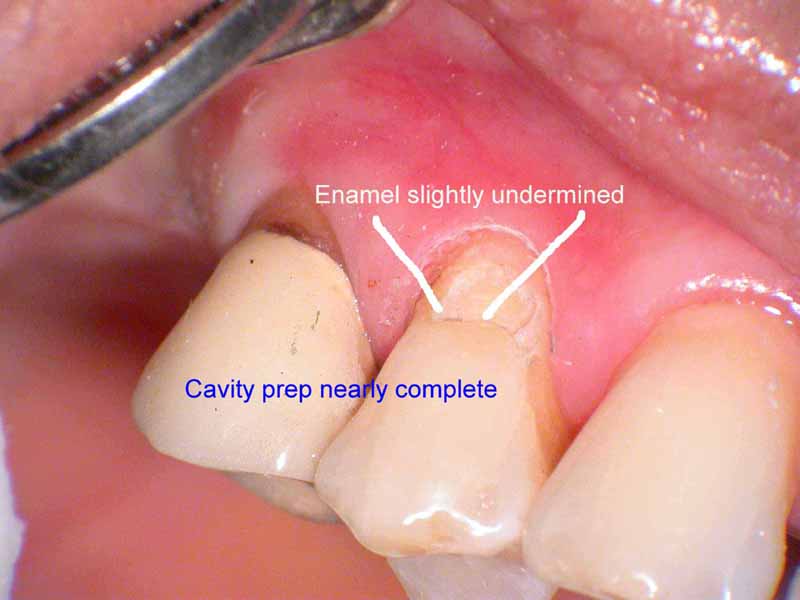
Distal area has been “prepped” using the Fr Nd:YAG at 100 usec, 3.00 watts, 300 millijoules per pulse (mj/p) and 10 Hz. Lasing was done DRY
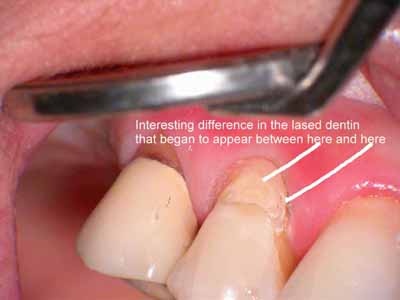
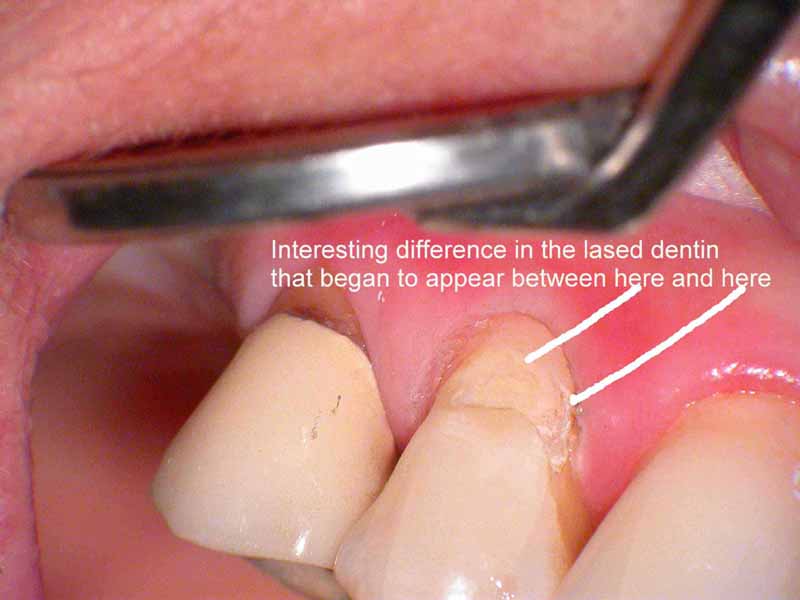
Continue removing healthy dentin, using occasional water spray from the 3-way air water syringe to remove any grey carbon (from plasma) or char that forms on the tooth surface
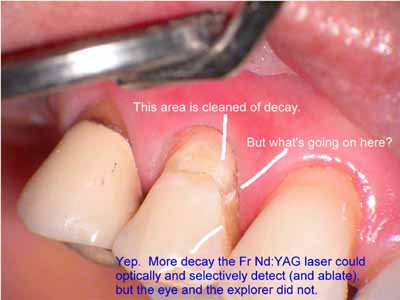
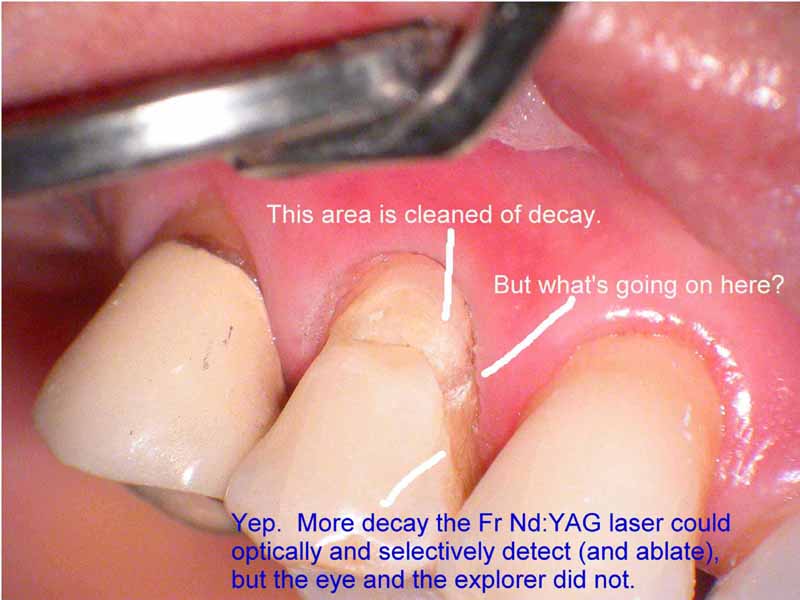
The selective nature of pulsed Nd:YAG–that “sees” different tissues with different tissue constituents, differently–allows for the tissue to ablate and appear different (Did you follow my thinking on that?) So now we have a different situation than I thought I had at first–which was to do a simple Class V. Now, because of the detection of decay in the dentin due to the pulsed 1064nm wavelength, I have a different scenario AND a different discussion with my patient.
Next to last image of my prep before bond and flowable composite with fluoride. Patient informed that a full coverage crown wil be needed if the dentin around the gingiva does not remineralize. Put patient on Prevident 2x’s per day.
Bob
Robert GreggParticipantHi All:
I posted this in the Nd:YAG section as well, but I wanted all the folks interested in “hard” tissue to see what pulsed Nd:YAG users have been doing for over 13 years.
This sort of Class V and tissue prep has been–and still is–routine stuff for us pulsed Neodymium users. We don’t require simultaneous water spray or anesthesia to accomplish this sort of result either.
Just thought all you dedicated hard tissue laser users might appreaciate what a dedicated soft tissue laser can do on dentin and decay using a properly configured laser with optimal (and variable) pulse parameters.
Thanks Big Time to Ron and Glenn for helping me get these images fixed up too! (Ron, I enlarged them to 800 pixels wide to show more detail. I think a happy medium might be 600?)

Above Figure: Used 4.0 Watts and 20 Hz, 100 usec PD to trough the gingiva from distal to mesial and accross the facial to expose the margin of the tooth, obtain hemostasis, and control the egress of gingival sulcular fluides.

Above Figure: Distal area has been “prepped” using the Fr Nd:YAG at 100 usec, 3.00 watts, 300 millijoules per pulse (mj/p) and 10 Hz. Lasing was done DRY.
Above Figure: Continue removing healthy dentin, using occasional water spray from the 3-way air water syringe to remove any grey carbon (from plasma) or char that forms on the tooth surface
Above Figure: The selective nature of pulsed Nd:YAG–that “sees” different tissues with different tissue constituents, differently–allows for the tissue to ablate and appear different . (Did you follow my thinking on that?) So now we have a different situation than I thought I had at first–which was to do a simple Class V. Now, because of the detection of decay in the dentin due to the pulsed 1064nm wavelength, I have a different scenario AND a different discussion with my patient.
Above Figure: Next to last image (ran out of memory on my card) of my prep before bond and flowable composite with fluoride. Patient informed that a full coverage crown wil be needed if the dentin around the gingiva does not remineralize. Put patient on Prevident 2x’s per day.
Bob
Ps. I’ll get a bigger card ASAP. Hey, I’m a Newbie at photos!
AnonymousSpectatorGreat pictures, Mark, thanks for posting.
How about going further and show some class II’s on permanent teeth? Still finding these frustrating. Not the prep part, but rather sensitivity. Today, did 20 DO and 29 DO but patient still had quite a bit of sensitivity (did refuse offer to numb up, though). Bathed buccal 30 sec, lingual 30 sec, occlusal 30 sec all at 5.5W 90/75. Started removing marginal ridge defocused and slowly moved into focus. Once to dentin dropped to 3.25W 60/40.
Continued to drop down all the way to 1.75 W 40/30 as patient complained of sensitivity. At that low a setting it was taking forever and a day to get anywhere.
Got any hints or tips?
Thanks,
2thlaserSpectatorThanks Ron,
First, I really advocate changing your settings to have a 30% differential air to water, it really speeds the cutting process. Also, I start really doing a slot prep more than anything else, if I can’t do a tunnel prep. There is usually so much enamel there, you continue to anesthetize as you ablate the enamel, with virtually no sensation at all, at least in my hands. Really focus the bathing to the occlual surface, directly, and SLOWLY into the central groove to maximze the thinnest part of the tooth for penetration of the laser energy. Once into dentin, I automatically drop to 2.75-3W, without really changing air/water…I keep the air at 80%and the water at 50% the whole time, unless lots of discomfort. Seriously though, I really don’t get much or any discomfort…lucky I guess. It’s funny you mentioned the class II’s because this morning I was talking to my staff about trying to do the same type of pictures with that in mind. I have to just figure a time to get it done. Great idea, (great minds huh?). Call me Ron, if you have any other questions…sometimes it’s easier on the phone.
Sincerely,
Mark
dkimmelSpectatorMark, Kept your photos in my head this morning while trying to do #15. It took like 10 times of forever at 5.5W 90/75. Dropped to 2.75W forgot the A/W setting for dentin. No sensitivty. I did the 90 sec deal a couple of times. Puzzled by the aamount of time it took.
I checked the tip undert the scope and the end was fine. The end that goes into the handpiece did have the white coneshape area.
Changed the tip and the next patient blasted trough a premolar in record time. The assistant was blown away. Cool.
Thanks for the picture it really helps.
David
2thlaserSpectatorDavid,
Cool. Glad to see you learned about where to look at the tips. I tell you, it really IS fast if you know what you are doing. (Not that I know what I am doing most of the time!). I guess alot, contemplate alot…then just do it. I take notes, then learn, and then share with y’all. Thanks for the nice posts.
Mark
2thlaserSpectatorJust want to welcome Chris Walinski to our forum! Chris we haven’t met, but I hear great things about you…please share here! We all enjoy things from each other!
Sincerely,
Mark
ASISpectatorHi Bob,
Under what magnification are these photos taken? Nice documentation. Would the decay that is not evident be detected by caries indicator or the Diagnodent?
I have also made the plunge into the scope world with a 4-step Global.
What do you think of the colour of the photos? A little faint?
What do you think? Glenn.
Regards,
Andrew
Glenn van AsSpectatorHi Bob………nicely done, they look good , a little washed out perhaps but all in all pretty darn good.
Bob, did you have it on aperture mode for the pics. just wondering and by the way…..NICE CASE.
Grin
I am getting worried that pretty soon everyone will be shooting scope photos……..
‘
FIrst Bob then Andrew……….OH MARK OH MARK……where are you MAAAAAAAAAAAARRRRRRRKKKKK.Glenn
Robert Gregg DDSSpectatorHi Andrew,
Yeah, they do look washed out. I’m playing with the settings and the image size still. With lots of help from Ron S and Glenn.
Here’s another sizing so that you can see closer up–the color and wash-out is still something to work on:
http://www.rwebstudio.com/cgi-bin/ikonboard/topic.cgi?forum=25&topic=76
Yeah, maybe caries detector or Dianodent would have worked. But as you look at the first image, there was no hint of decay to me initially. The patient will return in a couple of weeks and I’ll put some indicator on and see what it looks like. I don’t have a Diagnodent.
I used .66 magnification with I think is 4x. Glenn?
What’s the translation for those numbers on the 5 Step anyway (and why in the heck doesn’t Global just replace or add the mag number on the dial?!)
Thanks Glenn for the very GENEROUS remarks. I’m getting better thanks to you, Ron and Ralph Klink. I’ll check the aperture mode. The pics have some noise (ISO now at 200) and color issues still.
Don’t worry TOO much Glenn, in takes a while to get used to the scope in general before positioning the camera in addition to that.;) I’ve had 5 years or so with the scope so I know how to position the scope, steer it, fine focus it, hold it steady, “nose it” around, then take the picture.
But this IS fun:cheesy: , and outstanding for sharing clinical concepts, technique and technlogy of lasers and scopes. And because it is so easy to take the shot through the scope while working–instead of stopping to get the 35mm–there will be fewer missed opportunities to share clinical surprises like the one exampled here……
Thanks for the feedback, I appreciate it.
Bob
PS You know, I guess I should add and point out that the dentin looks white because it has been etched with the Nd:YAG. It melts and resolidifies dentin 60-100 microns deep and chemically as well as mechanically alters the dentin by removing the inorganic components and increasing the amount of mineral content.
(Edited by Robert Gregg DDS at 10:09 am on May 15, 2003)
Glenn van AsSpectatorHi Bob: depending on the length of your objective lens (200mm or 250 mm) and your eyepieces (most are 10X, but can be 8X or 12.5X mag) the .5 turret is 4x mag and the .66 is about 6X mag.
The magnification changes alot ………..depending on your objective and eyepieces.
For instance if you have a 200mm objective lens and 10X eyepieces than each number is multiplied by 8.
If you instead have a 250 mm objective lens you multiply each number by only 6.3. Its quite a difference for instance if you take the 1.25X tur ret spot and multiply by 8 you have 10X mag but if you only multiply by 6.3 then you have around 8x mag.
The 8X eyepieces will lower the mag again and the 12.5 X mag raises them.
It really is amazing to not only see the cases through the scope but to photograph them. Look how power Marks recent photos of how to prep a Class 1 with the laser are because of the closeup.
I am sure that with time he will get a scope and a camera, because the ease with taking photos right through the scope is unparalleled.
Cameras and scopes take a while to get the sweet spot.
I will ask Eric if he has any PDF files for using the Xmount adapter for the scope with your Nikon 4500.
Glenn
Kenneth LukSpectatorI’ve just registered today and am very excited reading through each post.
My patients normally would have had their hygiene appointment before examination. In this way, the fissures are generally cleared/ reduced from stains. 40 or above would be treated with Air Abrasion/flowable composite/ hybrid composite in deeper cavities. Fluoride treatment would be prescribed for cases between 20 to 40. Fissure sealants are not used at all since I would not be able to check these areas again in the future.
Kenneth LukSpectatorHi guys, Just joined the forum today. It’s great to see so much enthusiasm and inputs into laserdentistry. I don’t feel so much alone now as I’m the only one using the 980 in Hong Kong.
I’ve only been using the 980 for a few months. Would you guys please advice on the protocals in treating perio cases? Thanks! -
AuthorPosts