
Forum Replies Created
-
AuthorPosts
-
Robert GreggParticipantHi Everybody,
Here’s a case I had to deal with today on an uxpected basis. Patient had a C/C of sore gums. At first I used air and vacuum (to cool and for comfort) Fr Nd:YAG at 3.00 watts, 20 Hz and 100 usec pulse duration without local anesthetic.
[img]https://www.laserdentistryforum.com/attachments/upload/Eva1.JPG[/img]
After giving Lidocaine 2% with Epi 1:50,000 I tried again at a higher wattage but same PD of 100 usec. No such luck in getting hemostasis.
[img]https://www.laserdentistryforum.com/attachments/upload/Eva2.JPG[/img]
After anesthesia, I used a long pulse duration setting of 650 microseconds. Since I had disrupted the tissue and capillary vessels (opening them up), it took a little more effort and energy to get the area to calm down.

This is the kind of control over the tissue and bleeding that is possible when one can vary the pulse duration of a near infrared pulsed laser. Note the lack of char, zone of coagulation, or epithelial peeling. No post op recession for this patient………
[img]https://www.laserdentistryforum.com/attachments/upload/Eva4.JPG[/img]
Starting off using a longer pulse duration on hemorrhagic tissues avoids disrupting the tissue and
vessels with high peak powers of short PD (1500 watts per pulse), and getting immediate hemostasis, thus saving time & less irradiation exposure to tissue, i.e. proper “Light Dose”. Less chance of thermal injury to tissue that way through economy of energy.May 22, 2003

This is the missing Pre-Op x-ray showing the defective restoration.
This is the 7 day post-op. NOTE: Any recession or loss of tissue height?
Bob
(Edited by Robert Gregg at 4:38 pm on May 22, 2003)
AnonymousSpectatorHi Ken,
I think you might find these threads interesting re:perio
http://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=32
and
http://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=25
Welcome aboard!
Robert GreggParticipantNo reason to buy a pulsed Nd:YAG for the following reasons, but if you have one, here’s how you can use it for selctive removal of hard tissue components.

Pulsed Nd:YAGs with high peak powers of 3000 watts per pulse at 100 usec and 10 Hz are highly absorbed in calcium containing hard tissue and pigmented decay.
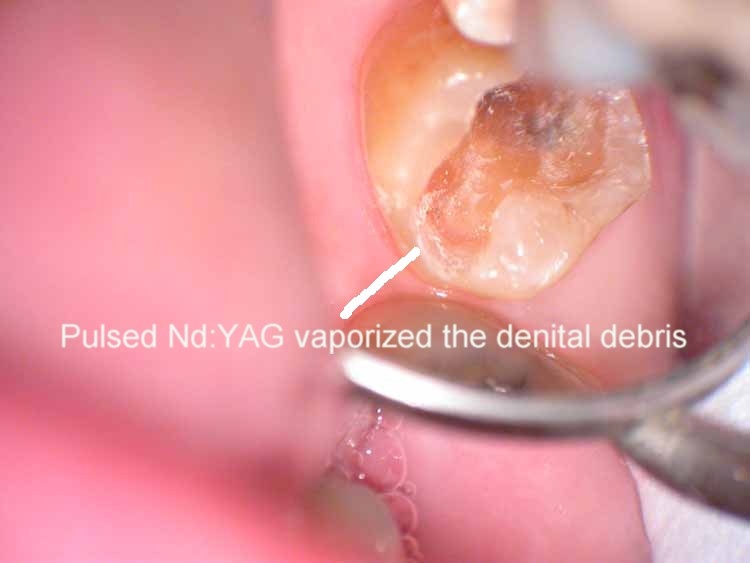
Very nice selective removal of dentinal debris, (without water or air, and defocused at a distance of 4-6 mm.

Yeah, I saw the fracture line on the DL. And so would the pulsed Nd:YAG too–see the next image for an even better demo of that through enamel and dentin.
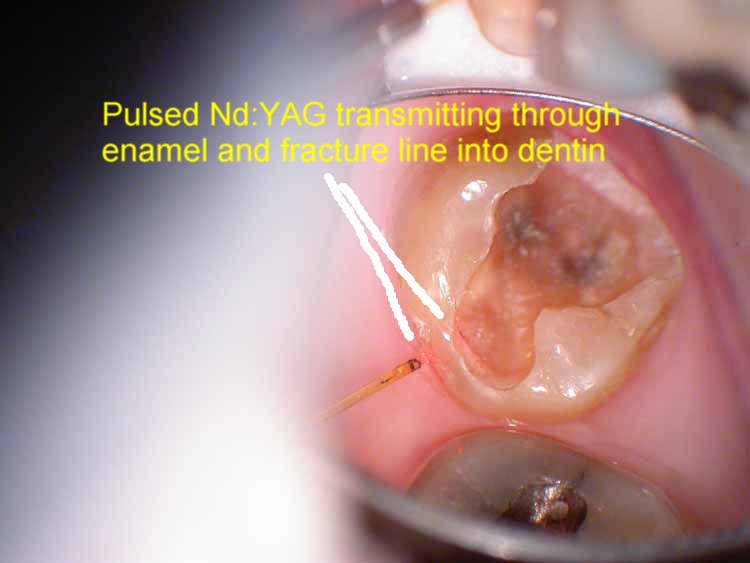
I don’t have the greatest cleave in the world, but I do have a very high energy density to transmitt through enamel and reach dentin on the other side with enough intensity to have absorption on decay on the other side.
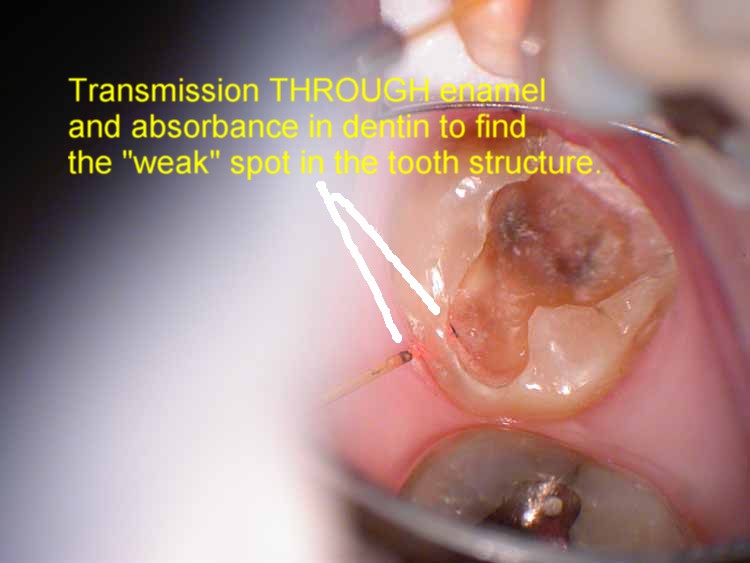
Self explanatory

Almost ready for impression for IPS-EMPRESS after I remove the decalcified enamel on the mesial and the fracture line on the DL margin[/b]
This making any sense to anyone??
Bob
Kenneth LukSpectatorThanks Ron,
Lots of info.
Sounds like I should have got the MVP instead of the 980.
Ken
ASISpectatorHi Bob,
Interesting application for hard tissue procedure.
Thanks for sharing again.
Andrew
Glenn van AsSpectatorCool case Bob and very interesting to see how pulse duration can affect hemostasis……I learn something everyday.
Can the long pulse duration also be done without anesthetic.
Was there a difference in pain perceived between the two sides.
Glenn
Robert Gregg DDSSpectatorThanks Glenn,
You can use long pulse durations w/o anesthetic if you are careful. Especially when you can select 250, 350, 450, 550 and not be limited to only 650 as your long pulse setting.
More exposure time = more chance for pain. And the exposure of 650 is 6.5 times longer than the very short 100 microseconds PD.
But most of the time, when the tissue is this messed up, it’s time to numb and get the job done, which is what I did.
Bob
Robert Gregg DDSSpectatorThanks Andrew!
Just fun stuff we’ve used our pulsed neodymiums over the years.
They are complimentary to erbiums in that they can be diagnostic in many ways on hard tissue and then an erbium can be used for ablation of diseased or damaged enamel and dentin.
I’ll post an example of this idea later today…..
Bob
Robert Gregg DDSSpectatorWelcome Ken.
Nice to have you on board and participating!
BOB
Kenneth LukSpectatorIntervention at #40 or above. I’d use air abrasion, using the diagnodent to check on cavity wall and floor. When there is little or no reading, I’ll restore with flowable composite; flowable/hybrid in deep cavities.
#20to#40, Topical fluoride treatment,review the sites 4 monthly. I don’t carry out fissure sealants so that I can review these sites.
Generally, fluoride treatment immediately after restorations.
Ken
dkimmelSpectatorMark what are you doing with bombed out teeth with old leathery caries. I am not having much luck. Takes forever. Your spoons are great in these areas but I was hoping to do more with the laser and just do a final check with the spoons.
By the way you are going to kill my budget next month. I was using the composite placement instrument this morning and its great. It is just thin enough and just stiff enough to work the interproxiamls.
Thanks, my wife is going to kill me.
David
2thlaserSpectatorDavid,
Actually I use teh laser…usually at 2.5-3W and keep penetrating the decay. What I notice is that the decay losens up from underneath and you can get it out in once big scoop using the #5 or #6 excavator. I then resterilize and fill. I do use the laser, and so far, it’s not too slow for me at least. When we get them real desensitized, it’s easy.I am glad you like the instruments. I REALLY like the placement instrument, as you say, it’s great for shaping interproximal areas prior to curing. It really cuts down on my finishing time. Glad to hear it! (I need a scope, I need a scope,…)
Mark
Glenn van AsSpectatorHahahaha……..the scope bug is like a bad flu bug…….it catches everyone in the room.
I think its great that people are beginning to realize the value of magnification for laser dentistry.
The scope is alot of fun for documentation and for providing the treatment.
All the best…….
Glenn
Robert GreggParticipantGlenn,
Ralph has me set at S Shutter 1/125
What up with that?
Bob
Robert Gregg DDSSpectatorGreetings All,
I will post the pictures when I get to the office later today, as I had planned to do yesterday. Del and I have a lecture today and I’ll have some time to upload the images.
In the mean time, some may want to see the reaction I got on Dental Town while trying to show and share the technical applications for plused Nd:YAG.
Instead I got grief over the necessity of care–something I never tried to address in the first place.
Thanks to Ron Schalter who made a much appreciated supporting post and made my technical point–it was about what the 1064 laser could and couldn’t do.
And thanks to David Kimmel who hit the nail on the head (borrowing from “Doctor Ed’s” hammer analogy) when he also posted and made a very important point about aggresive carious lesions in the elderly due to medications, dry mouth, poor saliva flow, and the inability to detect carious invasion into dentin using radiographs.
The caries extended 3mm into dentin! Talk about being surprised! I was expecting the stain to blow out and be left with healthy enamel. It started out as a simple case of stain removal–one reason I didn’t charge the patient is because I didn’t prepare her for the fee in advance. Oops. But again, that wasn’t the point I was trying to make….I wasn’t trying to make a statement about these sorts of class I situations. There’s the Congress of Microdentistry, Kim Kutsch, Stu Rosenberg, and others to make that case.
Anyway, thanks or the support, guys, it’s greatly appreciated.
Now I know what Glenn van As means about the hostility to technology and his previous clinical posts on Dental Town!!! Geez, just trying to share technical capabilities and some differnt ways of solving clinical problems and some of those people get TWISTED about it!

http://www.dentaltown.com/idealbb/view.asp?sessionID={DC5AF088-EE75-477D-A1D6-81103B24213A}&topicID=16692″ target=”_blank”>http://www.dentaltown.com/gold….
http
-
AuthorPosts