
Forum Replies Created
-
AuthorPosts
-
smileagainSpectatorRon
I am going full cycle on using my Diagnodent- first I did not trust the readings- I guess natural scepticism to a new diagnostic tool. Then I saw that there were also many low readings and this comforted me because I did not feel that we were finding many restorations that did not exist before. Now I seem to get readings of 0 to 4 on teeth that I am able to probe and stick with a sharp explorer and the “moment” sometimes goes to minus one or two. It “seems” that a higher reading should occur. Does anyone else get this kind of response?
I do calibrate often and take a test reading on a healthy tooth as directed.Any response would be helpful
With thanks, Jerry
Glenn van AsSpectatorHi guys…….off to Kansas to lecture……one last reply before I go (in 4 hours).
Al: your questions are always so darn astute. The camera is mounted to an arm that connects to the scope. See the pic I included below.
The treatment is illuminated via a xenon light source that connects via a fiber optic to the scope itself shining light along the same pathway as the eyes see.
I just get my assistant to push the shutter down while I hold the scope. There are remotes but the Nikon ones dont work too well.
THere is a foot control one , I am looking into it as we speak.
Hope that helps…..Glenn
As for primary teeth ROn……I have no idea but it sure works well on them. Only the really wimpy kids need anesthetic. It cuts fast and well in my hands on kids teeth which is where I use it aot.
Hi Bob…….I am not up to date on all the PD stuff and dont even know where my 3 year old paper manual is anymore.
If I find it I will look it up…..not sure of that though.
Glenn
Glenn van AsSpectatorHere is a scope pic or two… the last two show the camera, the first one shows the light source and the cable which plugs into the scope for a very bright light.
Glenn
[img]https://www.laserdentistryforum.com/attachments/upload/fiberoptics.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/Camera and scope.JPG[/img]
Robert Gregg DDSSpectatorHi All,
After Ron S., Del and I chatted about the different appearances in these similar lesions, I have a few thoughts:
1. Fibromas are not very vascular–being made up of mostly collagen. Erbiums cut collagen very well. So using an erbium with water and in contact will cause a nice CUT through the collagen fibers.
2. If you pull hard on the fibroma and streeetch the fibers out–THEN cut through–when the fibroma releases there will be more of that “crater” appearance (which I try to obtain).
3. Ron K. has demonstrated a very EXCELLENT technique of using the erbium to replicate a “punch” excisional biospy involving the peripheral borders.
Since Ron has gone into deeper, and therefore more vascular tissues with much LARGER capillary diameter than in and near the fibroma proper, AND using a none-hemostatic wavelength to include the margins for histologic assessment, there is much more tendency to bleed (but almost ZERO Zone of lateral thermal Injury). When Ron defocuses, turns off the water, uses light air to blow the pooling blood away from the capillary ends, he can get enough HEAT to char the surface (like a CO2 laser). That get him his hemostasis (along with a little pressure for the deeper aspects of that capillary bed). The thermal wound “injury” is very superficial–even though it looks crispy, it feels very comfortable to he patient as the c-fibers nerve endings are coagulated (necrosed).
My 2 cents…….
Bob
Kenneth LukSpectatorHi all,
As an absolute beginner with laser, I tried laser perio treatment on a friend of mine 2months ago. We carried out SRP 6 months before without much improvement.
Here’s what I did:
LA given,
Bolitec 980 , irrigating handpiece with saline irrigation into pockets at 4W 0.05sec on/0.05sec off, 15sec per tooth.
SRP,
Relase pockets with same parameters.
2 months after treatment, she returned last Saturday with pocket reductions from 9mm to 3mm. Lingual areas of lingually inclined lower molars showed the least improvement/no improvement ( 3 pocket sites ). All other areas improved to 3-4mm pocket depths.
Now I know I should have waited longer before checking up on the pockets.
She was very happy before she heard about the pocket depth improvements. She said she could feel a vast difference with this treatment.
Am I just lucky with this case?
It couldn’t be the SRP as it didn’t improve much after the first course of SRP.
Ken(Edited by Kenneth Luk at 12:03 pm on May 22, 2003)
Robert GreggParticipantSee above editions/additions.
Robert GreggParticipantHi Ron,
“Do we know excactly why primary teeth seem to “numb” up more profoundly than permanent teeth? Or is that just how it seems to me…all the best …………. “
We have always felt that it was BIGGER, JUICIER, HEALTHIER pulps that were more able to be effected better?
 ?
?Bob
Robert GreggParticipantAl–
I’ll say that was PEAK powers………any biostim effects for the tree?
Bob
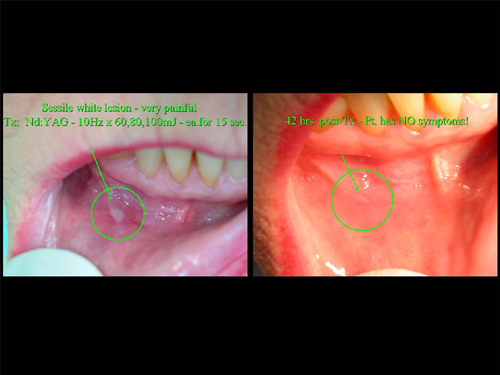
kellyjblodgettdmdSpectatorHello out there: An elderly woman arrived at my office two days ago with a lesion in her buccal vestibule – very painful, even deep into the tissue. Orajel wasn’t helping and her physician suggested she see her dentist. I treated the lesion with my Pulsemaster 600 Nd:YAG: 10Hz w/ 60mJ, then 80mJ and 100mJ each for 15 sec. Patient returned less than two days later with almost complete resolution of the lesion and all symptoms gone. She is a skeptic no longer.
Hope every one has a great weekend.
Robert GreggParticipantNice service Kelly. Nice photos too.
Can’t do a nicer thing for your patient!
Hope you charged her for that, or made a big deal for her about the “high-end” level of service you make available to your patients through technology that is unique to your practice…….??
Bob
kellyjblodgettdmdSpectatorThanks, Bob. As a matter of fact, I did charge her for this Tx. (贄, I think?) I was really taken back by how skeptical she was prior to treating this lesion. I have done fillings for her in the past with the Waterlase, which she enjoyed. But she just couldn’t understand how a laser could fix her soft tissue if her Orajel couldn’t. I suppose that using lasers is always a learning experience – for provider and patients, alike.
SwpmnSpectatorVery nice service, Kelly.
That’s an apthous ulcer, right? The Nd:YAG fiber contacts the tissue, right? Was there any need for anesthesia?
Have any theories been proposed or investigated regarding the mechanism by which laser stimulation causes resolution of these painful lesions?
Was the Pulsemaster 600 Nd:YAG made by ADT? Does it have user-selectable pulse durations? Happen to know what pulse duration you used to treat this lesion?
Thanks,
Al
ASISpectatorHi Kelly,
Looks good. How long have you had your Pulsemaster?
I like the photo of you with your baby girl. How old is she now? I have a 21 month little guy. Max keeps us pretty busy.
Andrew
kellyjblodgettdmdSpectatorAllen – Great questions. To the best of my knowledge this was an aphthous ulcer, so I treated it as such. The fashion in which I treated the lesion was based on research I have read supporting the biostimulatory effect of lasers. Most of my information comes from the text by Jan Tuner and Lars Hode: “Laser Therapy”.
I actually used the Nd:YAG in a defocused manner, approx. 1cm away from the lesion. The patient noted no discomfort, heat or any other symptoms. Quoting from their text regarding aphthous ulcers: “…The sypmtoms of most patients can be alleviated by laser treatment, and the healing period can be reduced. Carbon dioxide, Er:YAG and Nd:YAG lasers can also alleviate symptoms if a defocused beam is used. The dosage is determined by the patient’s response to pain relief. When the patient feels a distinct reduction in pain, you are on the way to the ‘right’ dosage. Several treatment sessions are often necessary to prevent any discomfort to the patient until the aphthae have disappeared. 4-6J is a good ‘starting point’.”Some literature they quoted from:
Fagoni V et al. Use of HeNe soft-laser in 32 cases of mouth aphthae. Laser Abstracts (Rivista Europea di Laser Terapia Medica e Chirurgia). 2 (2): 25-29
Takashi K. Clinical evaluation of a GaAlAs semiconductor unilaser irradiation on solitary aphthae erosion and hypersensitive dentine. Shikwa Gauko. 1987; 87 (2): 295-.
Colvard M, Kuo P. Managing aphthous ulcers: laser treatment applied. J Am Dent Assoc. 1991; 122 (7): 51-53.
Howell R M et al. The use of low energy laser therapy to treat aphtous ulcers. Ann Dent. 1988; 47 (2): 16-18.
There are more articles, but you get the drift, I’m sure.
To answer you question with regards to any theories being proposed on mechanisms by which this effect takes place: There appears to be two ways that low level laser therapy affects the tissue to which it is being appied.
First, there are certain cell functions which are stimulated locally (where the light hits the tissue – “primary response”). It is known that chromophores in the form of e.g. porphyrins, play an important role.
Secondly, there is a systemic effect, well shown through the use of CO2 lasers as biostimulators. Since the wavelength of CO2 lasers cannot penetrate tissue more than a fraction of a millimeter, there is no primary response outside of the outer part of the dermis. The stimulative effect, therefore, must therefore work through a secondary response.
Chapter 11 in Tuner & Hodes’ text goes greatly into the theory of biostimulation. They talk about how laser therapy is not based on heat development but on photochemical and photobiological effects in cells and tissue.
The Pulsemaster 600 is/was made by ADT. I can’t say that I was terribly impressed with their company – I got very little support, but it was the first laser I bought and I didn’t know any better. I do like the laser, however.
Unfortunately, I do not have the ability to affect the pulse duration on my laser. I can only change the Hz and the mJ. I wish I had known more about other companies and their products prior to my purchasing this Nd:YAG. Perhaps I would have purchased one that was more adjustable. I have owned this laser for just over one year.I hope this helps. I can’t say enough about the Tuner and Hodes text. They have a few different texts out. I’ll try to find their website and post it.
Have a great Memorial weekend.
Kelly.
kellyjblodgettdmdSpectatorFor anyone who is interested:
Great information on low level laser therapy on <a href="http://www.laser.nu/index.htm
This” target=”_blank”>http://www.laser.nu/index.htm
This is the website for Laser World – the Swedish Laser Medical Society.
Enjoy!
(Edited by kellyjblodgettdmd at 3:06 pm on May 25, 2003)
-
AuthorPosts