
Forum Replies Created
-
AuthorPosts
-
Robert Gregg DDSSpectatorRon and Bruce,
Thanks for the kind words! Bring your Day 2 book back when you come for Day 4, we’ll fill in some of the blanks.
Bob
whitertthSpectatorwould someone clarify Biostimulation of leions? what lesions would u biostimulate? At what powers with each laser…ie, Waterlase/Erbium, Nd Yag, Co2 etc. which laser works best for what lesions…This is an important thread that I think would benefit the group with some more explanation…I think there is some research now with Biostimualtion of post extraction sites as well….Comments…. Regards to all
whitertthSpectatorGreat stuff….. Keep up the good work
Robert GreggParticipantHi Everyone,
There is NOT enough protective armour that Rod Kurthy could don on me, or flame retardant material that Glenn could loan me, or that I could put on, that would protect me from posting this on any forum but this one……
Here is a usual situation I find myself in, like today–treating an endodontic tooth with a undetermined, yet suspicious plugged canal orafice.
Again, this is NO reason to go and buy a laser, but if you have a pulsed Nd:YAG that you are using for another primary purpose….like perio;)….then this might be a useful adjunctive application for this type of selective laser wavelength.
Patient presented with lost crown and incomplete endo. (Patient has LOTS of issues we are addressing). He’s been living with this tooth partially aopened up, but the MB2 or Mesial palatal(?) canal was not located nor instrumented.
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT1a.JPG[/img]
Photo for orientation. Upper right first molar
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT1.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT2.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT3.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT4.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT5.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/RandyRCT6.JPG[/img]

X-ray shows file is aligned in the canal properly and apparently reached the apical working distance.
Bob
SwpmnSpectatorThanks for the clarification, Dilbert.
How about:
Has or will the laser pay for itself? Y/N
Al
mickey franklSpectatorI am about to get my new Waterlase deliverd to me next week and woundered are there any dentists out there who do perio treatment with the waterlase(I have not got a diode)?If so how do you do this and what do you charge for this?
Also when doing crown lengthening and reaching bone how do you reduce the bone avoiding the gum?Also can someone clarify “biologicl width”
Thanks
Mickey
SwpmnSpectatorThank you,
Al
SwpmnSpectatorWell hell, if it looks like a nail, use your hammer on it!!!!!
Rod says that getting crapped on after posting on DentalTown is your Badge of Honor. I’ve a good mind to post my one and only Er,Cr:YSGG crown prep case just for the fun of it. That oughta get ’em going!!!!
So at that particular setting, your 1064 wavelength is selecting what was formerly soft tissue in that canal? Now if you cranked up the setting it would bang up the dentin a lot more, right?
Pardon my dumbness but please explain the term EJECTA? That just the stuff coming out of the calcified orifice?
Nice photography. How’d you get so many pics in one post? I thought we could only get three, has that changed?
Thanks and thanks for help with the question on Glenn’s gingivectomy comparison.
Al
AnonymousSpectatorMickey,
A few threads to checkouthttp://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=21
http://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=32
http://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=6
I’m sure there are more.Try the search feature.
Should make for interesting reading:)
AnonymousInactiveBob,
Great pictures – you are really getting the hang of this Photo stuff. It shows very well the whole process – well documented.
To all,
The neat thing is I get to work with this guy!!! I don’t thank him enough in public for the camaraderie and help he is to me. To have a partner that brings out the best in you is tremendous. Thanks Bob!!
Now you all have this kind of “partnership” working for you in this forum. Looking back I think how lonely it was. I don’t feel that anymore.
SwpmnSpectator70 yo female presents with endodontically-treated tooth #8 percussion(+), Class I mobile, labial fistula. Endodontic consultation reveals labial horizontal and vertical root fracture. Implant crown presented, patient elects three unit FPD(7-9).
After obtaining profound anesthesia with 4% articaine, an Er:YAG 2940nm laser was used to excise soft tissue 7-9 and then provide osseous relief apical to the labial fracture on #8. A 600 micron 30 degree quartz tip was used with distilled water irrigation at 100 mJ, 25 Hz, 250-300 microsecond pulse duration. Application time two minutes.
Forceps and a straight rongeurs were used for the extraction. Although the crown/core/root complex fractured into three, it was not necessary to reflect a periosteal flap. A three unit provisional FPD was fabricated.
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa052903-1.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa052903-2.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa052903-3.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa052903-4.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa052903-5.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/williamsa052903-6.JPG[/img]
Robert GreggParticipantHoly Cow!!! Al, you nearly gave me a heart-attack:o I was having a bit of Deja Vu all over again! Geez….you’d better be LAUGHING, cuz I’m biostimulating my heart to get going again!
Ok, compose myself………
Yes, at the 1064nm wavelength, and with the High Peak powers we can get at 100 microseconds pulse duration, 3.00 watts, 10 Hz = 3000 watts per pulse. Whoo aaah!
At about 2mm defocused, that engery will vaporize organic junk, and etch the pulpal floor dentin, but not vaporize calcified deposits (like pulp stones, for example) or remove dentin unless I decrease the “spot size” and get closer to the hard tissues.
At about 1mm defocused at this setting, the calcified tissue will vaporize before the dentin will. When I TOUCH the dentin, it will THEN vaporize, like in my previous post about Class V dentin prep.
Ejecta would be that material that is vaporized (in a gaseous state–such as carbon=smoke), small bits and pieces of what is being broken down, like calcified crumb bits, and dentin pieces. Really anything that is removed by “recoil” from the forward intense pulse hitting and being absorbed in (thanks Del) the substrate, interacting, and causing that substrate to disasociate into component parts, gas and smaller pieces.
See if this image helps:
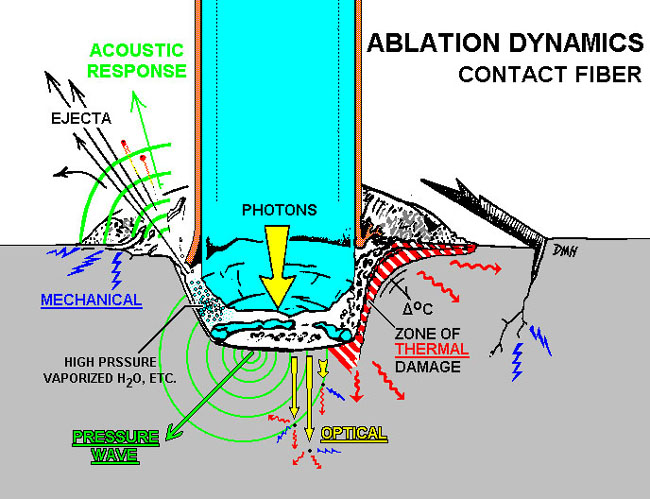
Image courtesy of David Harris, PhD, UCSF School of DentistryAs far as the pictures go, you just have to load them three at a time, unless you are MONSTER PHOTO YODA DUDE like Glenn van As who can create a collage and then just load one or two images.
Bob
Glenn van AsSpectatorHEY WAIT A MINUTE WITH THAT……
600 micron, ErYag, funny looking handpiece, 25Hz….what gives with that……
GIGGLE GIGGLE………
BIG GRIN.
Cool case and wonderfully documented…….
I love it for all the right and wrong reasons.
Glenn
Robert GreggParticipantAl–
What in the HECK are doing restoring a 70 year old to health. I mean, WHAT are you thinking?!
SNICKER, SNICKER. Just kidding Ron…..:biggrin:
VERY nice case, VERY nice documentation, VERY nice Photos, and VERY nice service…..
Bob
kellyjblodgettdmdSpectatorBob – fantastic case! I have a couple of questions:
1) Are you using a dental microscope for this?
2) I have an ADT Pulsemaster 600. I’m not sure what the pulse duration is, but, to your knowledge, does the PM 600 deliver enough energy to do similar selective removal?
Thanks
-
AuthorPosts