
Forum Replies Created
-
AuthorPosts
-
whitertthSpectatorwhile i I have been there before as well, next time u may want to try and drop your air amd water to no more than 20/20..sometimes that can make a big difference in the apteints feeling it or not…just a thought
Glenn van AsSpectatorI sometimes feel like I should have shares……..
Cracks are obvious with the scope……like decay , it is everywhere.
Thanks for the kind words Ron
Glenn
SwpmnSpectatorOIC so that’s where you use the soft tissue tip.
What kind of crowns are those, is that something like Procera or are those porcelain to metal crowns?
Al
Glenn van AsSpectatorI use the soft tissue tip for frenectomies, biopsies.
Procera crowns……..just for something different.
THe 2nd molar was a PFM I think. Thanks Al
Glenn
ASISpectatorHi Glenn,
Did you defocus for removal of amalgam or use local?
Nice work again.
Andrew
ASISpectatorGood work again, Glenn.
Funny how the #44 looks so good and virginal when the ones posterior to it are in such heavily restored condition. But after you are through with them, they look pretty darn good.
Are you finding that you favor the argon over the Diodent for troughing?
Andrew
Glenn van AsSpectatorHi andrew…….I used local.
I didnt know how deep it was going to be and I was in a rush as well.
Sorry Mark……but its the truth.
Glenn
Glenn van AsSpectatorHi Andrew…….I prefer the diode but I had to send it back and they are resending me a new one.
I had the one from the LVI meeting and they owe me one for all the work that I have done for them lecturing.
I am just waiting for them to finish production on a new batch. Mine was all in the box and then they were short 2 so mine got sent to someone in real need.
I like the diode better than my argon……less shrinkage in my humble hands.
PS thanks for the kind words, and yes it was so weird to see one tooth virginal and the rest filled to the brim like they were.
Glenn
Cya and really the Nd Yag or diode is a better laser for troughing I think than the Argon which chars a little and is a little deeper penetrating.
Glenn
kellyjblodgettdmdSpectatorJetsfan –
I know where you’re coming from. I find that for most people (who aren’t allergic to vibrations – haven’t heard of that one), most cavities can be done a reasonable amount of time, especially if the “anesthesia” of defocused energy is used. However, I also find that there are that group of people who are just easier to work on if they’re numb.
One question I have been asking recently is “Are you able to bite into an ice-cream cone” to assess how sensitive their teeth are in general. I find that people who are more sensitive normally also sense the laser sooner than other patient.
Although I love doing laser dentistry, especially when I don’t have to give a shot, I am now focusing less on not giving “the shot”, and making sure that my patient has a more comfortable experience, overall. If this means giving some anesthetic, that’s okay with me.Just my two cents.
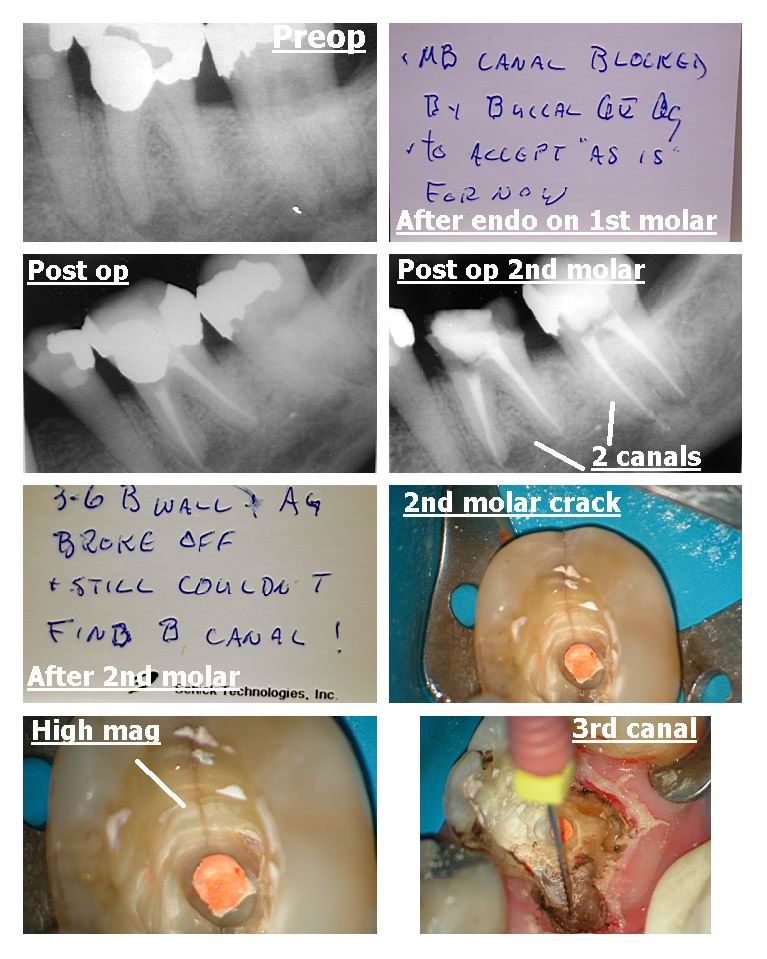
Glenn van AsSpectatorHi Folks: This was a weird case. Nice lady came in and needed two endos so she went to my local endodontist and his associate took on the case. This fellow just joined the practice but is an experienced clinician from back east. He had alot of trouble with both endos.
Only able to find 2 canals on both teeth….well I know more are there.The lady came in today with both temps almost all out (happened on the weekend) and a large crack asymptomatic in the 2nd molar and a badly broken down tooth on the first molar. It needs osseous and also lots of work to save it but first I need to temporize it and also find the 3rd canal on the mesiobuccal.
I troughed a little with ultrasonics and wham down it went. APex locator showed it wasnt a perf and that it was in the canal. At that point I wanted to isolate so I quickly built up by hand the case with Point 4 in the base which is a very plastic flowable. I used the Argon laser to reflect the tissue on the buccal at 1.0 watts CW and then quickly did a caries control type buildup to keep the saliva out.
Opened up the canal and put a temp. I am thinking seriously about going back and finding the second canal on the mesial root of the 2nd molar .
It has a big crack but its not symptomatic.
Cool case and on its way to endo, osseous, posts cores and eventually some crowns.
Only had 45 minutes ( less actually) to do something today so this is what we accoplished.
Hope you like it and you can see what a HUGE help the scope is……
I was proud of myself for this one today.
Glenn

2thlaserSpectatorGlenn, never any need to apologize. Sometimes ya gotta do whatchya gotta do! Nice though. I am finally back from 2 weeks of lecturing, need to get on the photo bandwagon now!
See ya all tonight!
Mark
jetsfanSpectatorKB,
I agree. I think many of us (me included, got caught up in the NO NEEDLE concept that we are willing to allow our patients some “mild degree of discomfort”.I am not sure if it is for me or the patient. On the one hand the patient does appreciate it when we are done and they have no lingering numbness. In fact they often say they would prefer to do it that way again, however, I do want to be able to deliver the no needle dentistry so I go to great lenghts to achieve this. But at the same time I am under a bit of stress, wondering if and when and how much the patient is going to feel.
PatricioSpectatorI am happy to report we are back in business. I did have a couple of patients who were unhappy to have the conventional dental tratment when the laser was down. This is the second unit with problems. The company took back the first unit. This surely is a piece of equipment we need to have working. The big problem is the delay in getting the technician in here to fix the problem. It seems to take most of a week.
Anyway we are doing fine now. Did a crown lengthening today with no L.A. cool. Going to get paid for it too. Feels so go when things are going right.
Pat
Janet CenturySpectatorHi Glenn –
do you know if there will be courses / discussions about both the DELight and the Diodent?
Thanks
Janet
Samuel MossSpectatorHi guys and gals,
I would hope that this could and would be a pivotal step in laser problem solving as far as the mechanics go. These are expensive little toys that seem to have peculiarities that are found out AFTER the financing has been set in concrete. ANYthing that could help us as end-users and possibly the manufacturers (do they REALLY want to know?) to improve lasers as a whole seems like a good thing to me. Or do I live in an unreal world?
Samuel R. Moss DDS -
AuthorPosts