
Forum Replies Created
-
AuthorPosts
-
jetsfanSpectatorI had a couple of people with cervical sensitivity, that was improved after using laser at .25W. However after a day or two they said the sensitivity came back. Suggestions?
PatricioSpectatorJetsfan,
I know there has been some discussion by Bob about elominating the neuroblastic tissues and biofilm on the tooth surface first from a distance and then closing the tubules at a closer range. Two steps. He also pointed out that occlusal interferences and bruixng can dampen success. He also pointed out that you must record on a scale of 1 to 10 the pain at the begining and the pain in your case the next day because the patient will interpret any pain as failure and not see pain reduction as success. How did I do Bob?
Pat
PatricioSpectatorMark,
I will want some individual instruments when they are available as a way of seeing what my needs will be. I will watch for more info.
Pat
Happy2thSpectatorQUOTEQuote: from Ron Schalter DDS on 7:04 am on Feb. 4, 2003
The ring flash is difused with whiteout (like you use for typing mistakes).What a GREAT idea!! My ringflash is almost too powerful for my digital camera and I think that this idea is going to be a godsend!!! Can’t wait to try it!
AnonymousSpectatorWelcome to the forum, Rich.
The whiteout works pretty well, you just have to be careful as the whiteout will scratch off. I’ve had to do a little touchup once in awhile.
jetsfanSpectatorPatricio,
thanks for getting back to me so soon.
I did it in two steps as was suggested at .25W. I did not get a 1-10 fix by the patient before and after, however I was able to infer from his comments. The next day he was at zero. A day later it was worse than the start. Perhaps the occlusion needed adjusting but I succumbed and placed a composite. Patient now out of pain, which is all that matters.
JETSFANI hope I don’t sound like I am knocking this machine. Quite the contrary I love it. I have done crown lengthenings, apico, endo, biopsies , aphthous ulcers, surgical residual root removals, sequestrectomies, operculectomies …..
But for routine , fairly deep class I , II anesthesia is unpredictable in my hands. Also desenstizing also unpredictable. So I try to pick the brains of all who have success. Thanks again
2thlaserSpectatorGlad to see you have got a nice camera set up Ron. Rich, Great to see you here, it was real nice to meet you in Vegas. Any questions when you get your laser, call!
Glenn, Hate to say it, you only beat me to the punch with the photos! I did a VERY similar case about a week before you posted yours. I have been lecturing in Dana Point and in Vegas, so I haven’t been on much lately. I had great results like you, and the healing is so darn fast. Patients LOVE that laser. How “quick” did the bone ablate for you in the smoothing process? When I use the Waterlase, it’s like a hot knife in butter, so I use very low energy settings, lots of water and air to keep the area clean of debris. Man, I can’t wait to get up and see you. I hope next month. Great stuff guys!
Mark
Glenn van AsSpectatorHi Mark………any time , just call in advance. I will be happy to have you come up and see the scopes and to see the waterlaser………I mean Delight Laser (grin)
I dont use mine all day like you but use it enough to make it very valuable.
Take care and let me know when so I can make sure I am not off lecturing.
Glenn
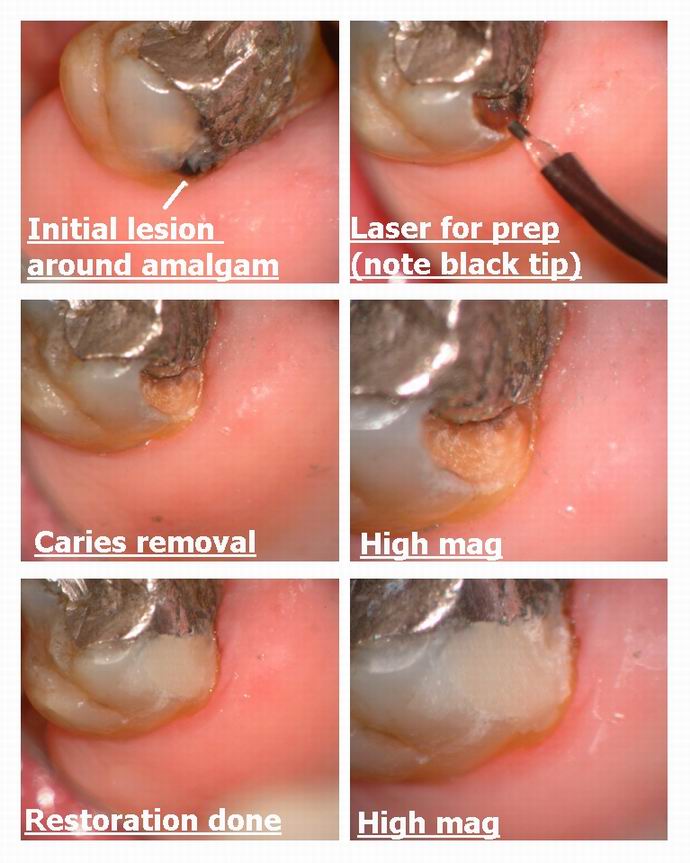
Glenn van AsSpectatorHi there folks: I did a simple Class V on the palatal of a maxillary second molar (we extracted the first molar around a year ago) and noted this decay. This lady is in her late 70s and didnt want anesthetic and has been quite ill , so I just did a patch on the tooth.
Note how the tip gets black from the amalgam and altough you cant cut amalgam with the laser you can work around it.
Photos shot through the scope, restored with Dyract Flowable.
Just something to look at……..
Glenn
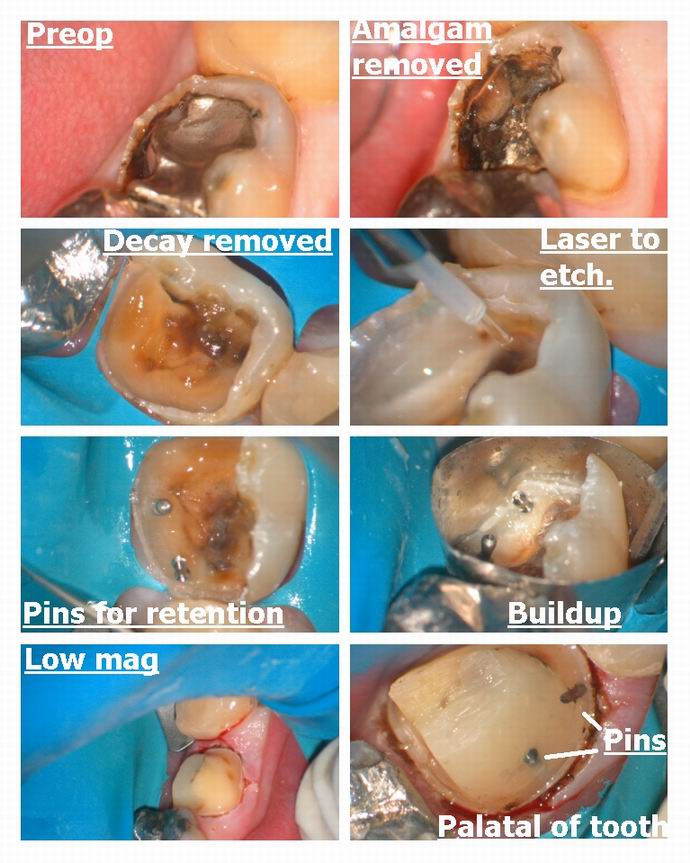
Glenn van AsSpectatorHi there folks: Patient came in and wanted me to fix the lower left 2nd molar today.
The lingual had fractured and there was ALOT of decay under the old amalgam.
I removed the old amalgam and wondered it was pulpal.
I got all the decay out but only a solid buccal cusp left.
I didnt know whether to do….
1. Large resin restoration
2. Pin retained core and crown
3. Endo plus post , core and crown
4. Large resin buildup , no pins and then crown.You can see I chose pins and a resin after laser etching the tooth structure. I have heard LOTS of people mention that pins may even weaken cores but I know that when I put them in on cases like this that the core NEVER EVER comes out during the impression or during the temporary fabrication.
I used the laser to help with tensile strength of the buildup and to sterilize the tooth.What would you have done……….I just can justify no retention but I am sure many of you do it daily with better success than me.
All the best……….
Glenn
Nuno FerreiraSpectatorHi
wend i start using my waterlase in Portugal, and because im the only one using a waterlase, the training and information was not enough so my patients refer very sensibility in laser procedures, i used to use anesthesya in 30 per cent of the cases.
Last year i spend some time learning and with Docter Chen and now im a very happy Waterlase user…sorry my patients are.
PatricioSpectatorGlenn,
I do not have a better way but I likely would have placed slots more or less where you have the pins for retention of the resin and I feel I would achieve the same result. Possibly this is slightly easier.
Pat
lagunabbSpectatorHi Glenn, and everyone else waiting for a copy of the paper:
Still have not received it yet and I haven’t forgotten. If I don’t get it by tomorrow, it will have wait till the week of 2/24 before I will get around to it. Sorry for the delay.
Glenn van AsSpectatorHi Ray………I sent it by regular mail last week.
Should be there but maybe not til next week.
Glenn
lagunabbSpectatorOk. I am skiing next week so it will probably be 2/24 when I get around to it.
-
AuthorPosts