
Forum Replies Created
-
AuthorPosts
-
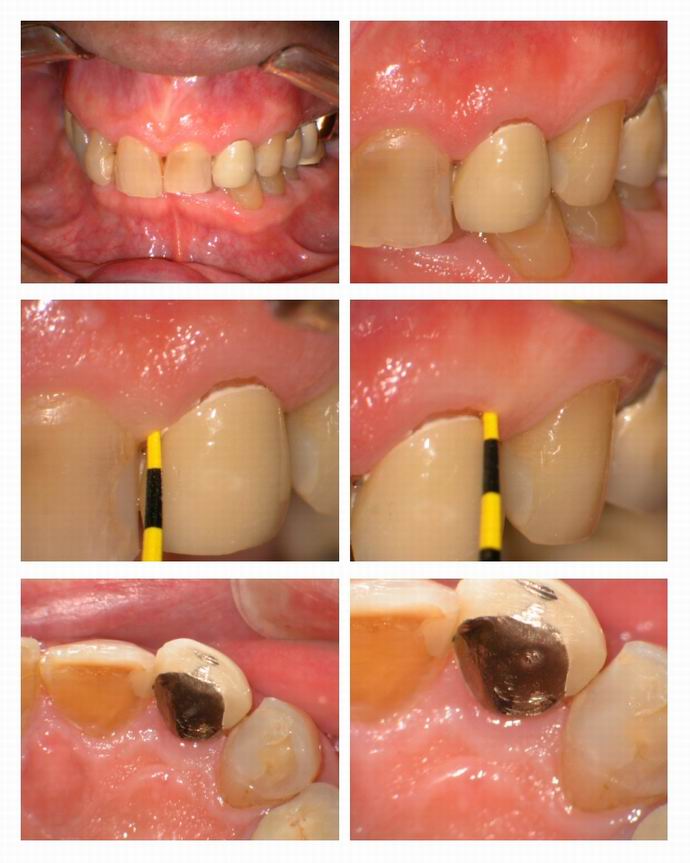
Glenn van AsSpectatorHi folks: Today I had this case where a patient had fractured a maxillary lateral incisor at the gingival.
My associate did the endo and put a post in the tooth but the crown didnt fit too well and there wasnt enough tooth to put a post and core on, particularly on the buccal (more on the palatal)
I did a crown lengthening today and used the erbium to cut the flap using the unique wedge type tip that Continuum has (amazing how little hemorrhage there was) and then raised the mini flap and removed bone with a 600 micron tip with water. I then actually reduced the flap height by using the laser to reduce the edge of the tissue, and then used the Argon at 0.4w to “tissue weld” the flap back together without sutures. You heat up the tissue so it gets tacky and draw the laser across the flap.
Laser periodontist Larry Finkbeiner showed me this a long time ago and it does work if you dont have the wattage too high.
I like the final result , will see the patient for photos tomorrow and show the healing photos…….
Got it all on video.
Hope you like it…….the flap I cut with 30 Hz and 120 mj without water.
I cut the bone with water at 30 Hz and 90 mj.
Flap reapproximated with 0.4 watts Continuous
Glenn


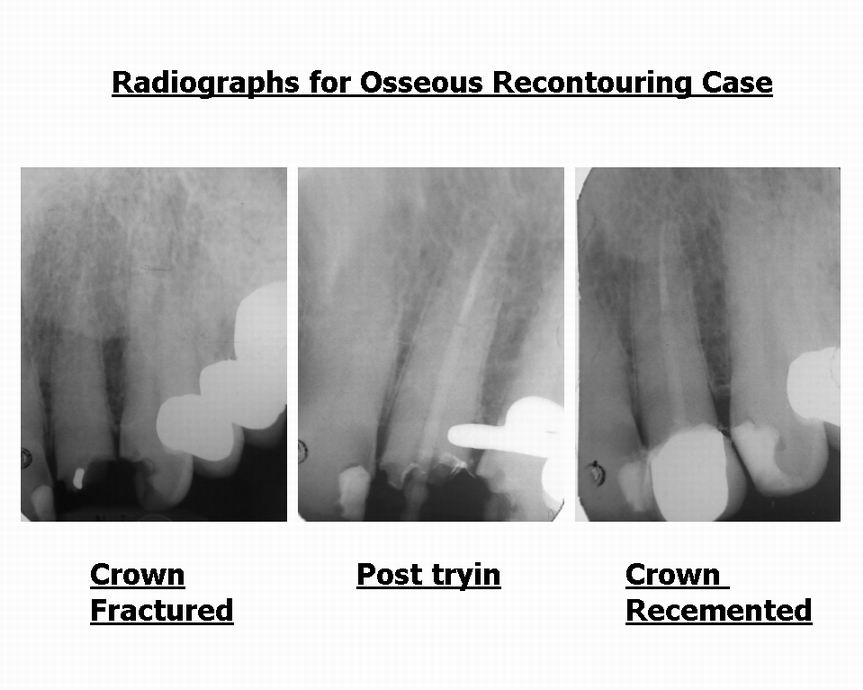
Glenn van AsSpectatorHere are the radiographs from before I started the case.
Glenn
PatricioSpectatorJetsfan,
Thanks for your comments. What a great group of contributors. I am sure this board will make significant contributions to the clinical effectiveness of lasers. I am thinking in my hands that certainty is uncertain. The predicability comes in the bag of tricks which experience brings to the table. For example in those deep sensitive spaces simply moving to a slow rotating high torque round bur in the electric handpiece does it. If this is not the case then intra osseous anesthesia will almost always cure the discomfort in a few seconds and it is back to the laser. The cure all that ends all marketing of the laser is probably not true. At least not for me. Thanks for sharing your experiences the info moves up all forward.
I did my first significant case of reverse bevel gingivectomy yesterday with the biolase. It was easy and I can see it will improve our results in those deeper pockets. I seem to get good results at 1.5w pre set with a G6 tip somewhat defocused. Just close enough to cut. Little to no bleeding and no charing. The tissue seemed to look good when I was done. I wish I had one those slick camera systems to share my beginnings.
Pat
AnonymousSpectatorPat,
How about more details-
Pocket depth
scaling/root planing 1st?
Goal of the procedure- removing inflamed tissue inside the pocket?/decreasing amount of attached gingiva to reduce pocket depth?/zapping the bugs?- some ,all or none of these?Next steps- when recall? when probe again?
Thanks for sharing your plan of attack and why.
(Bob Gregg’s training me well, wouldn’t you say? ) 😉
Glenn van AsSpectatorHi Pat…….there are some very good cameras that are digital which could really help you in taking photos.
Canon makes the G3 and you can get a macro lens and diffuser (type of flash system) from Photomed or Norman Camera and make and EXCELLENT camera for a reasonable price.
I think that photography has made me a better dentist, in that it has allowed me to look back at my cases ( especially with the ones taken through the scope) and critique it after the fact . I can and often do look at the pics at home and then decide what I could have done differently.
It really is amazing, and getting constructive criticism from others makes you even better.
My suggestion is go out , get a camera and start taking before, during and after pics.
Glenn
Robert Gregg DDSSpectatorPat–
You said it better then I did!
Ron–Training?? I’ll show you training soldier–at 3 days of Laser BootCamp!:biggrin:
But I like the questions for more detail, to be sure! Good going!
I surmise from the technique and description that Pat was dealing with little inflamation? I futher suspect an occlusal component to the defect–hence the lack of bleeding in and around the pocket.
Jetsfan–desensitization takes time and patience. Occlusion is more of a contributing factor to all sorts of problems than I ever thought in my first 10 years of dentistry–and I had Peter Neff as my instructor at Georgetown. He’s now at Pankey.
Resist the urge for instant gratification…..
Bob
(Edited by Robert Gregg DDS at 11:43 am on Feb. 14, 2003)
2thlaserSpectatorBob,
Your words of wisdom are always so great, thanks for all you do for us “newbie” laser users!
Mark
Robert Gregg DDSSpectatorThanks Luke,
Remember to use the Force.
OB
Janet CenturySpectatorI took the Proficiency course just before I bought my lasers. Given my patient base, I thought it was important to have the paper on the wall. Most of the people at the course had been using their lasers for a long time.
Janet
AnonymousSpectatorQUOTEQuote: from Robert Gregg DDS on 11:41 am on Feb. 14, 2003Ron–Training?? I’ll show you training soldier–at 3 days of Laser BootCamp!:biggrin:
That would be awesome! The trade in value of my Twilite Diode towards the nd:Yag and training is?
 ???
???
PatricioSpectatorRon and All,
I use a comprehensive non surgical approach where we apply everything we know to best effect. We work toward top quality oral hygiene before we begin and every step of the way.We pretreat with an antimocrobial for one to two weeks prior to sc/rp. This reduces inflammation, sensitivity, soften calculus and greatly reduces bleeding during sc/rp. We don’t really root plane as in the olden days but get the roots as free of calculus as possible. We try to complete sc/rp phase in care in two successive days. We continue with the antibacterial for four additional weeks of healing and follow up by the hygienist, then the good doctor evaluates, usually I check and rescale any pockets still over 4mm and reassess the total picture. I then rediagnose and retreatment plan and this is where I am inserting the laser for any pockets of 5 millimeters or more. I am opening the pockets by beveling so the irrigant can reach deeper into the pocket area. I reduce the pocket height where possible to four millimenters or less. In many of these cases we use special periodontal appliances to deliver the irrigant at night and along with a daytime protocol so we get nearly 24 hours of tissue contact each day. A problem for the appliances is pumping the irrigant into pockets were the gingivitis has reduced and created a purse sting effect at the collar trapping the infection within the pocket so the laser should open this up and help us out. Since I just started I have nothing to report as to results but should have some early impressions soon as I have done two cases this week.
Three of us Biolase users are following a similar protocol. One was a speaker at the Dana Point meeting but not on perio. We have taken training through the Xerostomia Society which is the source of the product and appliances. http://WWW.drymouthdentistry.com
PatGlenn,
I confess I do have a Kodak D290 with a ring flash. I use to daily for facial pics and anterior cosmetic views but haven’t used the flash. I need to applying myself to learning how to take pictures and all the stuff you do. I have had a picture of myself for a few weeks for this board but have not done anything with it due to lack of experience in this area. Just one more mountain to climb.Bob, thanks for the back up and additions
Pat
PatricioSpectatorGlenn,
Once again these visuals are very helpful to me. Thanks for posting it.
Pat
2thlaserSpectatorHey Ron, How do I get more “red dots” and become a full memeber! I notice people are passing me up!
Mark
Robert GreggParticipantRon,
Call me. I think we can work something out……..I have a little pull aorund this joint.
Bob
Robert H. Gregg, DDS
Private Practice
President & CEO
Millennium Dental Technologies, Inc.
10945 South Street, Suite 106-B
Cerritos, CA 90703Home: 714-960-9910
MDT Office: 562-860-2908
Fax: 562-860-2429
Cell: 562-577-2454
Email: rgregg@millenniumdental.com
<a href="http://www.millenniumdental.com” target=”_blank”>http://www.millenniumdental.com
AnonymousSpectatorThanks Bob,
I’ll come see you at the ALD meeting and see what we can work out. -
AuthorPosts