
Forum Replies Created
-
AuthorPosts
-
dkimmelSpectatorBob, Ok you got me on the hook!
David
Robert GreggParticipantDavid–Just funnin’ while I remembered where I put those references…..
Here’s a great one for everyone to start with:
1. Dr. Paul Bradley’s video from the 1999 ALD meeting in Palm Springs, “Current Status of LILT”. #039
Very informative, very well presented and entertaining.
Contact Joyco MultiMedia and ask for Bob or Joy (tell ’em I sent ya’) at P: 303-421-0093; Fax 303-403-9112
2. Low Level Laser Therapy by Tuner and Hode available from Dr. Larry Lytle of Lasers, Inc. 605-342-5669. Good book. Larry is also a great sourch of information.
3. The Science of Low Power Laser Therapy
by Russian researcher Tina Karu available at Amazon.com for ๳.95 (used to be around 趚).” target=”_blank”>http://www.amazon.com/exec….ooks
Karu’s book is by far the most scientific and also the most dry…….
Larry Lytle is usually at the ALD meetings and is always very fun to talk to. Ask him about “proud tissue”.
Bob
Robert GreggParticipantHi Ron,
This is an occlusal/orthodontic/perio problem in my opinion. Look at the bone loss on the distal of the molar, and consider the absence of the second molar in the occlusal scheme of disease.
Like Rod said, it needs splinting and most likely endo.
Are there anaerobes to be dealt with. I’d say so.
Rod has studied perio a lot longer than I have, and knows a lot more about it than I do.
I agree with Rod on no pre-surgical S/RP 100%.
I also agree with Rod as to splinting (i.e Ribbond).
And I agree with the likihood of endo (with a qualifier).
But I would not (probably cuz I can’t) get as elaborate as Rod would.
I would treat the pocket with a pulsed Nd:YAG, use peizo electrics to lightly debride the root surface, make sure I developed a stable fibrin clot using my laser of choice………
Then I’d leave it alone for 9 months.
Here’s some stuff previously published in Dentistry Today, but with a new unpublished color graph of each probing site as they healed over 27 months. It helps one to appreciate the 3-D aspect of these defects. There are no “distal” bacteria, nor “mesial/mid-root” bacteria.
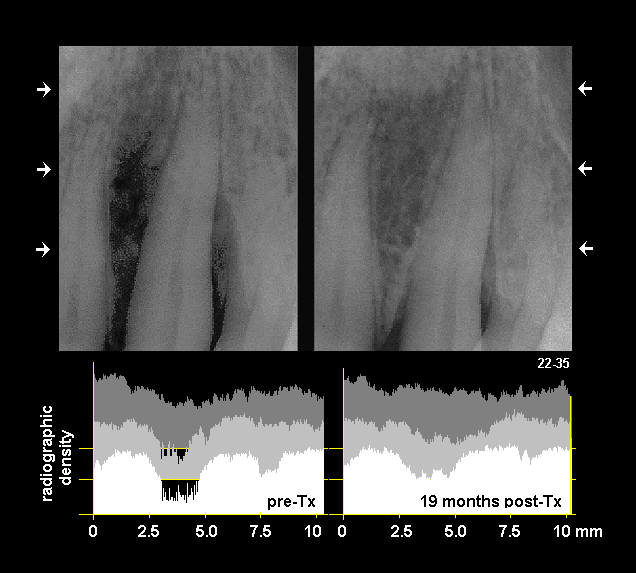
This tooth was treated only once in the first 9 months. The “mesial” defect was 19mm and the “distal” defect was 16mm.
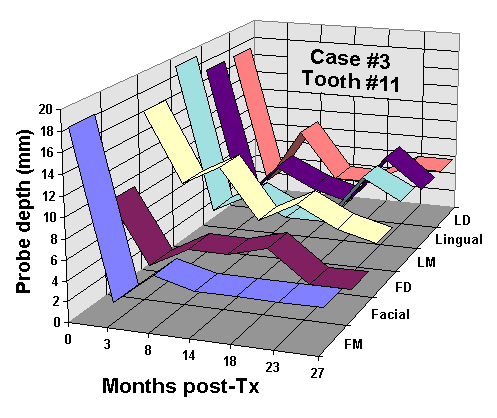
This color graphic shows the pocket reduction for each of 6 probing sites over a 27 month time frame.
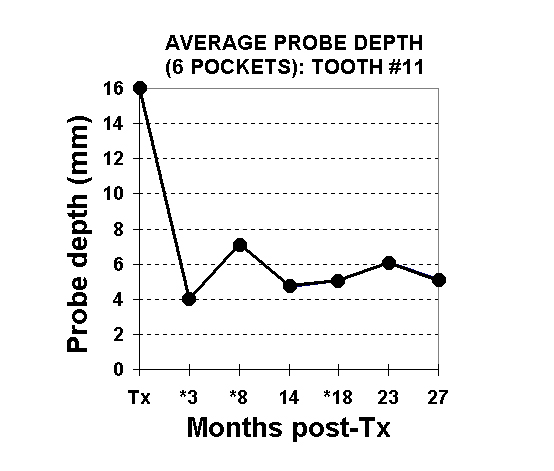
This graph depicts the total of all 6 probing depths averaged at pre-treatment; and the average pocket depths over time.
What is interesting, is that healing of periodontal defects–regardless of the method employed, tend to show a similar “rebound” effect at 3-6 months (a reverse “hockey stick”).
What was of great interest to us, is that use of LPT kept the pocket depths stable over 27 months without retreatment (except for the distal 6mm which was retreated 3x’s over 4-5 years).
Bob
(Edited by Robert Gregg at 4:43 pm on Feb. 19, 2003)
SwpmnSpectatorMan, is this not the coolest thread or what? We gotta get the word out so people can see these images.
I don’t know jack about engineering, but I’m going to go out on a limb and propose a theory:
Biolase developed a “handpiece” delivery system because they knew this would feel very familiar to dentists. If anyone ever looked at the ADT Cavilase it was developed similarly with a “handpiece”. Problem is, you can’t bend a trunk fiber 90 degrees, so Biolase put a mirror in the “head” of the handpiece to reflect the laser beam down the tip and into the treatment area.
Unfortunately, the mirror gets burned or pitted when one touches a metal-containing restoration/base/liner because as Mark said, the laser energy is reflected back up the tip and onto the mirror. As the dentist continues to use the instrument, the outgoing laser energy hits the damaged mirror and is reflected back into the trunk fiber, thus resulting in trunk failure.
But why use a “handpiece” mirrored delivery system at all? The shape of the handpiece casing is what was designed in the 1950’s to contain air turbines or the same as is now used in electric handpieces for gears. I don’t like the laser “handpiece” because it is hard for me to see around the “head” – particularly because it is set at 90 degrees unlike modern air/electric handpieces.
Crawling further out on the limb:
Glenn’s ConBio DeLight trunk fiber does not fail because there is no mirror(although there is an optional “handpiece”). Glenn uses a “pen-like” delivery system, looks similar to an electro/radiosurge unit(he showed me diagrams). I propose that in the ConBio DeLight the trunk fiber does not fail because there is no mirror and the tip acts like a “shear pin” or “weakest link”. When the tip is damaged there will be a reduction in cutting efficiency but no mirror-reflected damage back into the trunk fiber.
Just a crazy theory. Ya’ll let me know what you think and let’s continue this great dialogue!
Al
2thlaserSpectatorAl,
I am with you on this one. I think you are absolutely correct as far as the Biolase design, and reasons behind it. I have seen a straight handpiece they have developed, but don’t know if there is a mirror in it. I would think there isn’t, wouldn’t make sense to need one. I know I would use the straight handpiece quite often. I don’t think that the energy from a pitted or blackend mirror reflects back, but instead, the energy has no where to go, so IT backs up, heats up, and then the fiber goes. I will find out from Andy, as I will see him in Salt Lake on Friday during my lecture, and I promise I will get back to all of you then. You are right, great thread!
Mark
2thlaserSpectatorHere is a picture of a tip, that has a split starting at about 8 o’clock, it runs from the edge of the tip to the inside edge. Very hard to see without magnification. THESE are the tough ones to see, shine your operatory light through them, that seems to help. (like transillumination).

Mark
SwpmnSpectatorMark:
That makes a ton of sense about a damaged mirror – laser energy backs up and burns out the trunk fiber. Personally I also believe it damages the internal components of the Erbium because I’ve had to have mine completely “overhauled”.
But I don’t want a “straight handpiece”. What I need is a 30 to 45 degree angled fiber end with a removable tip. I’ve contacted ConBio for more information and will look at the product in April at the California Dental Association Spring Session.
Keep us posted on what you learn.
Al
SwpmnSpectatorQUOTEQuote: from greg holm on 8:04 pm on Feb. 16, 2003
So, with Delight, you don’t get the black spot?
How much did that little black spot on the mirror in your waterlase hanpiece cost to replace and were you able to do so chairside?
If a Waterlase user, wouldn’t the smart thing be to remove all amalgam with a handpiece first before doing anything to the prep with your laser handpiece?
GregAfter your one year warranty period expires, you will be required to purchase a yearly service contract for the Biolase Erbium laser. Be careful to read the fine print and get it in writing that this covers the delivery system, e.g. burned out mirrors on handpieces. The current fee is 񘴘 per year. Handpieces are easily changed chairside. Biolase will send you new or refurbished handpieces the next business day and you will need to return old handpieces with damaged mirrors.
My suggestion would be to never use the Biolase Erbium around amalgams or PFM crown margins. Use of the laser in these cases will result in damage to your tips, mirrors, trunk fiber and possibly the internal components of the laser.
Al
Glenn van AsSpectatorI have had zero spark of matrix and it acclerates the cutting in class 2s which makes me think that it isnt the metal but actually the materials in the amalgam.
What say ye…………..
Glenn
Glenn van AsSpectatorContinuum has both a straight pen handpiece and a contra-angle handpiece.
I dont use the contra angle as with the scope its harder to see around.
I think the tips for the ConBio laser are around 50 us now.
In addition there is a metal sheath that the tips go into and this slides on what you saw in the pics.
The sheath comes off very easily and the tip can be slid inside it and placed in the Statim.
Glenn
Glenn van AsSpectatorI dont know how the contra angle works but it fits on the existing fiber.
Hoya is the company behind Con Bio and they are a fiberoptic company so guess what is the strong point of the laser………..the fiber.
They just dont burn out very often.
As for being careful, I am not so careful at all.
The handpiece is a cool thing for most but as I said for me it is a waste.
Glenn
socalsamSpectatorHi gang. as far as the crack, I would chase it to a reasonable depth. if you can eliminate it, great. if not, I would place a nice temp crown and evaluate the tooth in a few weeks.
Glen,
in your case (very nicely done by the way) why did you choose full coverage? could you have not done veneers or modified veneers instead??
Glenn van AsSpectatorTerrible treatment………..bogus.
I treat usually above 20-25 and its because I am conservative.
This is crazy.
Glenn
socalsamSpectatorguys,
these types of situations are all too frequent in my office. My best success has been with Tenure bonding agent and corepaste from denmat. The tenure is self cure as is the core paste. use your post of choice ( I try to stay away from metal, too many fractures) and you will get a great build up that is rock solid.
make sure you have an adequate ferrule effect and get enough of the natural tooth structure.
dkimmelSpectatorThanks Bob!
Sure will ask Larry about “proud tissue”!!
Sounds like getting some of my city friends to order Mountain Oysters at the local dinner!!
David -
AuthorPosts