
Forum Replies Created
-
AuthorPosts
-
BenchwmerSpectatorI’ve been a soft tissue Nd:YAG user going on 4 years, got an OpusDuo Erbium last month for hard tissue.
The touch screen/ computer techology, handpiece.wave-arm delivery system and the foot control to vary power during delivery sold me.
It’s a hard machine to get, I ordered at the ADA meeting in October. They set up a standard profiency certification class for me to attend, The laser was professionally installed, local rep came the following day to go over all settings, questions, etc.
The Erbium laser fits in well for my no amalgam/ Microdentistry practice. I use it in conjunction with Air Abrasion. Use the Nd:YAG for most soft tissue needs.
I’ve ben impressed with not having to use Local Anesthetic, even in deep caries cases or trimming the gingiva on Clas V preps or root desensitization.
Let me know if I can be of any help. I’ll be at the Academy of Laser Dentistry Meeting this coming Weekend. I’ll be able to get any answers there.
BenchwmerSpectator
Here is a picture of the OpusDuo Laser Center, I wanted the laser without the CO2.
Mine just has the Erbium laser.
Looks good.
BenchwmerSpectatorSince I started using Air Abrasion about 9 years ago all my sealants are prepared w/ microabrasion, bonded w/ DBAs, then restored w/ flowable composite,
If any stain or caries present I remove all resin w/ AA. Need magnification.[img]https://www.laserdentistryforum.com/attachments/upload/Before.JPG[/img]
See case:
[img]https://www.laserdentistryforum.com/attachments/upload/Before.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/After AA.JPG[/img]Note more caries present under intact sealant that unsealed grooves or failinf sealant
[img]https://www.laserdentistryforum.com/attachments/upload/Restored.JPG[/img]
Note dentin caries after AA. This is what I got Erb:YAG for for caries removal and disinfection.
I use a 7th generation DBA, I-Bond for 30 seconds, thin w/ air, No light cure yet.
Restore w/ flowable composite, vibrate out any bubbles, light cure.
Adjust bite, polish.
If after AA if not into dentin, charge out as sealant. If into dentin, charge out as a one surface restoration.
The bonding agents have changed over the years, but predictable, conservative, microdentistry.
lagunabbSpectatorHi Bob,
It’s been several months since I talked to Bill. Laser jocks still don’t know how ablation (not even considering the role of water) really works. Like I said to Glenn, they are finally trying to use simulations to understand ablation mechanisms. Look up the stuff being done at U. of Montreal by Danny Perez and Laurent Lewis. Until we can understand the simple case of laser ablating a uniform material, there will be no hope of complete understanding of tooth ablation. All I see is one dimensional experiments and guesses and debates of what is happening and not much else. We will still be here debating 10 years from now if we depend on for-profit companies to fund studies. Thank the lord for the physics folks that are looking at industrial applications and doing fundamental laser research. There are plenty of pseudo-scientific types in the medical laser field drawing all sorts of meaningless conclusions from useless experiments. Gosh, did I get too blunt again. Sorry.It was a beautiful day at the beach.
Glenn – forgot to answer your question about stalling out in deep trenches. Below the threshold ablation rate, Neev’s work indicate you start to get into all sorts of problems associated with heating so that would be consistent with his model.
(Edited by lagunabb at 8:22 am on Mar. 3, 2003)
SwpmnSpectatorDr. Kimmel posed to me a question regarding eye protection from the Erbium laser if one is using magnification loupes.
Currently I have no protection as I need loupes to perform laser therapy so don’t use the provided safety glasses.
Can those of you who are using loupes or microscope and are in the know help us out and provide some guidance? What is the risk of using loupes with no filter for the Erbium laser irradiation? Can loupes be coated or altered or replaced so that they will have some sort of filter and provide proper eye protection?
Thanks for your help,
Al
AnonymousSpectatorAl,
I have filters that pop in behind the lens of the safety glasses that come with my loupes. They are wavelength specific. In the Laser Supply Forum there is a thread with links to Innovative Optics and Trinity which can make these. For the last pair (diode) I ordered the snap in frame from Surgitel and then sent it off to Trinity and they made the filters fit that frame.
I’ll try and remember to take a picture and post it tomorrow, of the filters for the loupes that I have.
AnonymousSpectatorAl,
I have filters that pop in behind the lens of the safety glasses that come with my loupes. They are wavelength specific. In the Laser Supply Forum there is a thread with links to Innovative Optics and Trinity which can make these. For the last pair (diode) I ordered the snap in frame from Surgitel and then sent it off to Trinity and they made the filters fit that frame.
I’ll try and remember to take a picture and post it tomorrow, of the filters for the loupes that I have.
BenchwmerSpectatorI ‘ve used Laser Clip-Ins for my Orascoptic Loupes for over three years. They fit inside the glass frames. Light grey tinted.
Recieved from Innovative Optics 800-990-1455
My inserts work w/ Nd:YAG, Diodes and Erb:YAG wavelengths.
BenchwmerSpectatorI ‘ve used Laser Clip-Ins for my Orascoptic Loupes for over three years. They fit inside the glass frames. Light grey tinted.
Recieved from Innovative Optics 800-990-1455
My inserts work w/ Nd:YAG, Diodes and Erb:YAG wavelengths.
PatricioSpectatorMy thoughts are like Glenn’s. We give our recare patients and experience and this requires time. My position is to consult, recommend treatment and evaluate the results which for perio patients often includes some rescaling of the deeper pockets by me.
I can scale along with other treatment and while waiting for something and in a business manner, and at a fast pace but this is not the experience I want for my patients.
I have done this plenty over the years when between hygienists and I always enjoy seeing the actual conditon of the mouth before the evidence is distroyed it does give and edge to diagnosis.
In some markets patients are willing to pay the doctor’s fee for the hygiene service and it can be given as a experience but for most practices this is not the case in my opinion.
Pat
Robert GreggParticipantHey Ray,
Not too blunt for me.
I appreciate the lead that Glenn took in causing dentists to think a little about science versus claims and hype. He took a lot of heat for that on Dental Town by a few “vocal” posters (not Rod), who said something like, “what does the mechanism matter, it works, so shut-up about it already!” Then in the next post say something like, “It works great because it is HK!! “It must be the HK, cuz no other laser works as good as this!” (Well, maybe it just might be that the pulse duration of 140 usec versus 300 usec might have a role……..???)
Neither Glenn, nor any of us, should have to apologize or back down for wanting to see the evidence that a proponent relys on to support a clinical or scientific claim.
Heck, for 12 years the periodontists and the AAP have been slamming and hammering us to show them the SCIENTIFIC evidence of using lasers in the perio pocket is better than SR/P alone. Not once have I felt those request were unreasonable–but it has taken time to do the research (by a for profit company).
QUOTEWe will still be here debating 10 years from now if we depend on for-profit companies to fund studies.Of course you didn’t mean EVERY for-profit laser company…….now did you? :biggrin:
It was a gorgeous day out! Here come da rain….
Bob
Glenn van AsSpectatorPhone Tom Barrows at Innovative Optics and have him make a filter for your glasses to drop behind them.
Erbium isnt as dangerous as Diode, argon or some of the others but it isnt good to not use safety lenses.
Argon is absorbed by the retina and causes problems there.
Erbium is absorbed by the cornea and lens which has water in it……..
Each individual wavelength has its own issues.
I have posted some pics before of laser safety options with the scope but ask if you want me to repost.
Look for Trinity or Innovative optics.
There are web pages for each I think
Glenn
Glenn van AsSpectatorPhone Tom Barrows at Innovative Optics and have him make a filter for your glasses to drop behind them.
Erbium isnt as dangerous as Diode, argon or some of the others but it isnt good to not use safety lenses.
Argon is absorbed by the retina and causes problems there.
Erbium is absorbed by the cornea and lens which has water in it……..
Each individual wavelength has its own issues.
I have posted some pics before of laser safety options with the scope but ask if you want me to repost.
Look for Trinity or Innovative optics.
There are web pages for each I think
Glenn
AnonymousSpectatorHi All,
Looked slow on the board this morning so I thought I’d add a little something.Xrays


Preop Picture
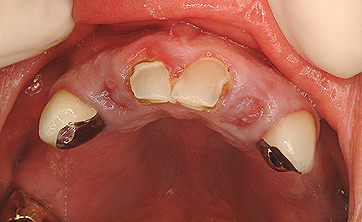
10 uncovered, 7 “outlined”
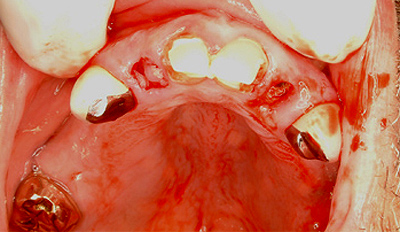
Post Extraction
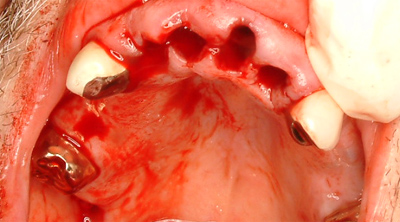
er,cr:YSGG
9mm perio tip
.75W 11/7 for tissue outline
4.0W 50/50 interproximal bone removal
Immediate RPD placed
lagunabbSpectatorBob, I can understand the AAP position given the early experiments using relatively high powers as you had noted on Dental Town and the implication of potential damage because of low absorption of 1064 nm in hydroxyapetite and water.
Speaking of absorption, Hibst stated something in his paper that pigued my interest. He wrote that hydroxyapetite has higher absorption at the YSGG wavelengths compared to Er:YAG. I had assume they were about the same. Know any references on absorption spectrum of hydroxyapetite?
-
AuthorPosts