
Forum Replies Created
-
AuthorPosts
-
SwpmnSpectatorWe appreciate your help Ron, Jeff and Glenn.
Al
SwpmnSpectatorWe appreciate your help Ron, Jeff and Glenn.
Al
SwpmnSpectatorNice case, Ron and great use of the Erbium to access the roots!!!
After interproximal osseous reduction, how did you extract number 7 and 10? Were you able to elevate the roots or did you use a particular forceps/instrument to extract these teeth?
Al
AnonymousSpectatorAl,
On #7 I removed a little bone on the disto-palatal and elevated the root out with a straight elevator. On 10 , even the 9mm tip was too short so I used an east/west elevator to remove a little more bone interproximally and got a purchase point and popped it out. I thought the neat part was that only the papilla between 7-8 was split, the rest were all totally or partially intact.
PatricioSpectatorHi all,
Glenn is on record as stressing the importance of magnification. I agree. I am presently using a Ziess 3.6 with light and am thinking about a second unit for another op. to use for comprehensive examinations as well as some treatment. I have read some of you are using 4 or 4.5 or maybe even 6. Maybe different strengths for different things. It seems to me I see quite well with the 3.6 but am wonder if some of you have progressed up in power say above 4 and feel you woud never go back, so to speak. What IS the working man and woman seeing through out there in the trenches? If this is not one of Ron’s survey questions it might be a good one.PAT
greg holmSpectatorFirst post for me in a while. We use a prophy jet and used to also use a disposable aa called airbrator to clean out grooves. we still use prophy jet but Graeme Millich who has a great cd on diagnodent told me the aa would remove too much tooth structure as well so we no longer do this.
Greg
greg holmSpectatorToday I removed a 5 unit brige with 3 abuts that had been in place for 30+yrs. #10 had been rc’d and had broken below the gumline.
I really wanted to keep this as an abut and add on #9 additionally.
I was also really sorry that I did not have my delight or waterlase as I sharpened up my machete and burs to crown lengthen around this area. Just kidding about the machete but I hope you get the idea
Tell me, would laser have been simpler for me and would there be less post op discomfort for the pt? Would healing time be shortened?
Greg
AnonymousSpectatorGreg, Graemes cd’s are terrific.
Is this the airbrator you’re talking about?

At บ -พ do you follow the single use?Easy to connect/disconnect? Mess?
Thanks
greg holmSpectatorRon. No we don’t. We have found that we can refill these ourselves with powder. The tubes or tips are wiped off between pts. these tips do wear out though and then we replace by purchasing new. These things do work. I mainly use them for cleaning out my preps. I have one set up in each op.
Greg
greg holmSpectatorBy the way the hose adapter(the metal coupler at the left in the pic) is about ๑? to get started too. But, I do
like these things. They work every bit as well as the Mach 4 I paid บK for in 95! I have since thrown the Mach 4 into the dumpster literally!
Greg
Glenn van AsSpectatorRon: Really neat pics……..clap clap clap.
I like the minimal tissue damage postoperatively.
Nice handling of a tough case.
Your making them a partial I guess.
Glenn
Glenn van AsSpectatorHi Ray and Bob……..you live and learn. Each day I come here I learn.
Granted some of my rants were beyond what most dentists care about but someone had to ask the question about where was the science behind HK.
Even someone as knowledgeable as Ray and Bob still ask the same questions.
ANyways, guys got tired of it. I worry thought that many companies are not as concerned about educating their users like Bob and Millenium are.
I dont own an Nd Yag but would be interested to read Bobs packet to educate myself to why the Nd Yag may be so good for perio. I know he has 7 pulse durations and that is good for decreasing pain during treatment.
I have said many times that I just want to learn more and each day I come here I do. My staff wonder if I lie awake at night dreaming up these uses for the laser but in fact its really not that. I learn so much from everyone here.
I hope that others who buy lasers may be like Ron , and Al (to pick on two guys) who didnt know that much in the beginning but became involved in learning , educating themselves and now know one heck of alot about lasers.
I commend those who come here repeatedly ( I watch to see who the active users are and what they are reading….thanks ROn for that) and I think that this forum is marvelous for education.
Thanks to all of you for putting up with my HK rants. I got put up to it from alot of my long talks with Tom Haney at Conbio about it.
Kudos to Biolase for taking the ads down and for their wonderful marketing ads (busty models aside)!!
Keep the threads coming.
Glenn
Glenn van AsSpectatorGreg: Like anything there is a learning curve and that is why I come here to try and learn more about how to use these items. Mark, Rod, ROn and especially Bob have really helped me alot.
AL and Pat have chipped in as well alot of times.
I think that the laser will make some things easier but the tissue will bleed and you will find it slower than a bur but it will heal very very nice.
Keep asking the questions and you will find answers.
Glenn
PS dont hesitate to buy one, market the heck out of it as in 5 years it wont be such a novelty.
Glenn van AsSpectatorPat………do you know what I am gonna say ……..you do dont you.
You need to look at scopes. At least explore that option. You can get scopes from seiler, global and zeiss easily in the USA.
There are other players but they are not as big…..ie Jedmed, Moller and a few others.
Designs for visions makes loupes , my preferences are Orascoptic which make 3.8 , 4.3 and 4.8 loupes ……
You need a light.
Mark (who is AWOL these days), uses 6.0X mag.
I am gonna post a case right here in a minute that I did today showing the value of high mag……not really a laser case although I did use it so that I can justify posting the case here.
I am lecturing here in Vancouver on scopes. 2 Years ago I did the same lecture and had 4 at the hands on workshop.
This year I am close to 30 for the same hands on .
40% of the sales are to GPs………I am not saying that you have to get a scope now but at least pursue it if you are looking at an upgrade.
Glenn
My scope case will be posted in a little while.
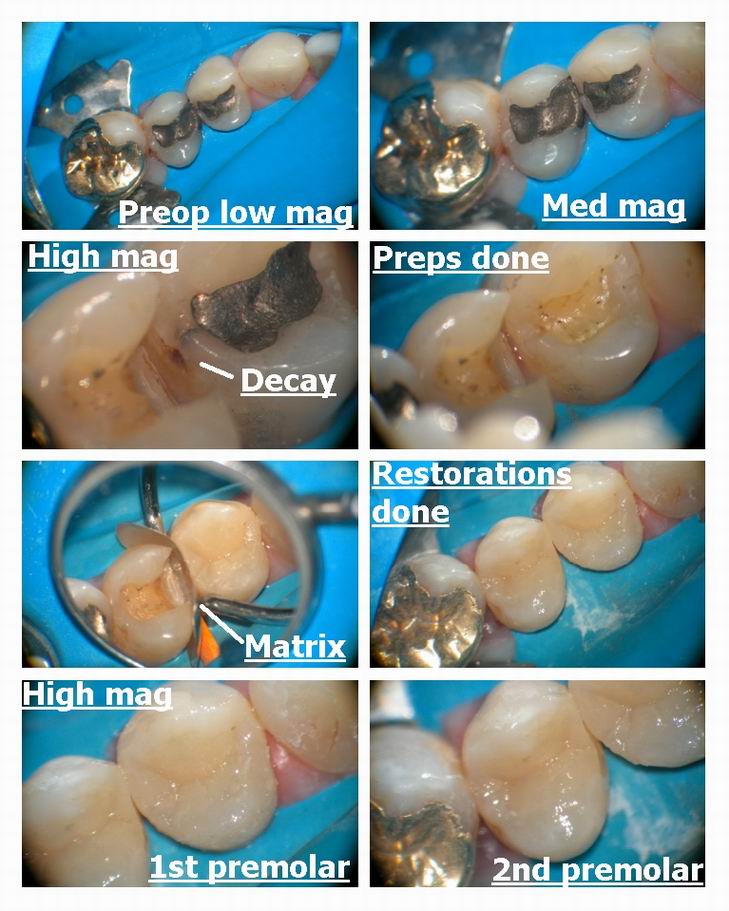
Glenn van AsSpectatorOk here is one case I did today (gosh digital photography is great isnt it).
Lady is awful to work on , she hates coming, sighing , moaning, making all sorts of sounds ( my hygienist thought I had someone challenged in the chair). The beauty is that I only see a tooth (no grimaces , faces etc) when I tune the person out looking at one tooth.
100% of my retina is on the tooth…I LOVE IT.
ANyways I prepare the MO on the 2nd premolar and darn it all see decay on the distal of 1st premolar. I did it and showed the patient afterwards……they never complain for two reasons.
1. with the high mag I can show the where the decay is on the photos on a 20 inch TV and zoom in on it.
2. The amalgam is gone and it is white.I hope you see the value of the scope in this one.
glenn
-
AuthorPosts