
Forum Replies Created
-
AuthorPosts
-
2thlaserSpectatorNice tip Pat. I have been out of town, guess I should read those other posts before I chime in! Hope everyone is having a great weekend.
Mark
PatricioSpectatorMike,
Welcome to the Board!
I ended up with a spare trunk in the beginning and I can be back in business in 15 minutes when I have a problem. Since I use the laser all day long and many folks want it that way I greatly apreciate that extra trunk. In my geographic location depending upon whien the trunk fails it might mean a full days booking would need to be shuffled or be willing to do it the old way. If I had to pay 񘴘 and I was using excellent maintenance procedures I might go with next day air plan and suffle the patients as possible. On the other had if I have a spare trunk and kept my schedule in tact, what are the risks of failure of the laser vs not having a maintenance contract for the second year as a means of paying for it? Something to think about.Pat
mike esposito ddsSpectatorThanks for the welcome Pat! So you have an extra trunk fiber and forego the insurance. Hmmm, interesting, but aren’t there a lot of other expensive parts that could break?
Living without the insurance contract is a bit of a crap shoot, isn’t it?
Mike
joesimmonsddsSpectatorI’m a newbie looking for practical help with some laser safety issues.
I am pulling together a lecture on lasers in dentistry to dental hygiene students and while dealing with laser safety made the mistake of reading, well, trying to read, the OSHA and ANSI laser safety regs. I was shocked by all the regs, apparently relating to much more powerful lasers in research, industry, etc, that, if adhered to 100% would make laser use in dentistry unrealistic. It brought up several questions which I hope some of you on the forum will be able to answer.
What type of signage are you posting in your office for Waterlase and LaserSmile units? Are you tightly restricting access to treatment rooms? Specifically for Waterlase, are you consistently wearing protective eyewear? (Physics lecture at Dana Point indicated that with great affinity/absorption for water at 2790nm and defocused diffusion of energy, distances greater than 5cm from tip were safe and that any reflected radiation would be absorbed by eye’s tear film.)
My staff and patients are always in protective eyewear but I am having trouble finding something useful with loupes. I have the clip-ins that, when placed inside the surgitel frames, make the whole thing weigh about 2 pounds! Very uncomfortable after any length of time.
I’d be interested in what types of practical applications any of you are are making regarding signage and practitioner’s protective eyewear.
Thanks,
joesimmonsddsSpectatorCertainly seems like a case of overtreatment. Like Pat, I will verify hygienist’s readings with my unit prior to commencing treatment and will only restore where those are >20. I have never NOT seen caries in teeth with readings above 20. Although, I’ve gone in to do several sealants (DIAGNOdent readings between 15-20) only to find significant decay deeper in the tooth (usually mandibular premolars) than normally seen.
Glenn van AsSpectatorDr. Tay was not overly impressed with these bonding systems especially for dual cure purposes.
I am not an expert on the bonding of porcelain onlays.
This one failed at the cement border, it was leaking .
Luckily it was salvageable and one of the few that wasnt pulpal…….most are just mush as you know when you get them off.
I know that putting pins in is frowned upon but I always am scared to place the core on dentin alone. Then you pull the temp of and out comes the core.
ALot of people do endo on these but I cant justify it if the decay isnt pulpal.
The tissue will heal nicely here, and I will take pics but your points are very valid.
Todays speakers included Bob Winter , John Kois, and Harold Heymann and sell as John Sorensen.
John is coming to the office tomorrow so I can show him the scopes as he wants to document procedures more and has been emailing me about scopes.
All the best and great points
Glenn
lagunabbSpectatorGlenn, received my copy of the paper. thanks. The pictures did not come through as you said. I would be interested in your PDF version if the pictures are clearer. Thanks again.
2thlaserSpectatorRon, where did you read about that case? Just curious. Because I think I just read a similar review. Just wondering.
Mark
AnonymousSpectatorMark, I sent you a PM. I don’t want to draw negative attention to the doc or the organization that published the article, so I won’t post that here.
Robert Gregg DDSSpectatorCoolness to the max!
Robert Gregg DDSSpectatorHi All-
Take a metal matrix into your “lab” and lase it. See what happens. In fact, do that with a lot of the materials you use in dentistry to better understand how they interact with any laser device.
Bob
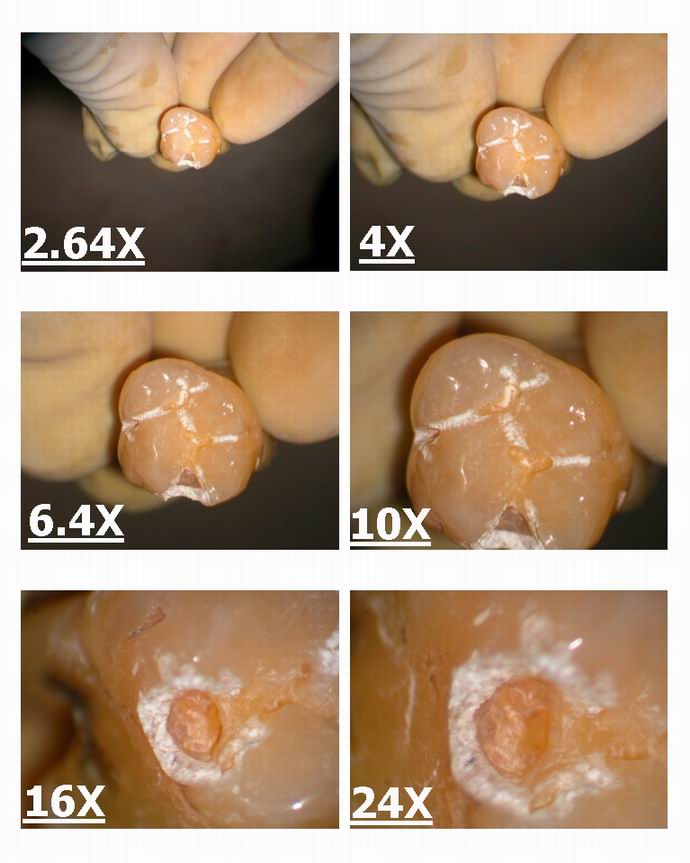
Glenn van AsSpectatorHi Folks: I have gone on record as saying that magnfication is very very important with lasers and I am going to post some photos and some cases to emphasize this concept in this thread.
Here is the first one showing the six different steps of magnification with my microscope and what you see on the same extracted tooth laser prep as the magnfication increases.
You can see the detail of the etch etc…….
You can see how the value of the scope for decay removal and for checking out how efficiently you are cutting is.
Glenn
Robert Gregg DDSSpectatorHi Glenn,
I don’t talk much about my bonding experiences since there are so many Gurus out there that speak reasonably well on the subject.
I started bonding DICOR to the dentin and enamel in 1985 using total etch. Learned from Ray Bertolotti.
I stopped using pins at that time too.
I learned on my own and with Ray’s help (John Kanca wasn’t anywhere around then) how to get those suckers to stick and stay without decay. Now I bond Empress to anything that ins’t deep sub-gingival, even second molars. “Deep anatomy” and occlusion are key.
If not a bonded Empress, then a PFM or FGC with a long bevel and no BU at all.
I have never been impressed with SE and don’t use it without a TE or laser etch technique thrown in.
Bob
Robert Gregg DDSSpectatorPerhaps Tom Haney can put his “clean copy” into a PDF file for all us interested folks?
Tom?
Bob
Robert Gregg DDSSpectatorWelcome Wiam,
What model Pocket Pro did you buy?
What training did you receive? CD-ROM? Hands on? Live patients? Category II/Standard Proficiency?
Will you be attending ALD in March?
Thanks,
Bob
-
AuthorPosts