
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorChris ……what does Sirona tell you. Do they have any information on their website.
Ordinarily the manufacturer knows best.
Glenn
Kenneth LukSpectatorI believe they do have footswitch as an alternative.
Ken
cadavisSpectatorThe manufacturer does not have an alternative handpiece. As I mentioned in my original post, I would prefer to use the footpedal that came with the unit, I just need to find a lightweight handpiece to hold the fiber. Since most diodes use similar fibers, I imagine that one of them will also work for the Sirolase.
I just wanted input from some of you who have other diodes that may have come with a plastic handpiece.
Kenneth LukSpectatorTry Laser Dental Innovations:
Howard Feinberg
howardf2@comcast.netKen
Kenneth LukSpectatorHi,
I want to incorporate Velscope to the office. Any users that can give me some advices please?
Ken(Edited by Kenneth Luk at 1:46 am on Jan. 16, 2007)
JasonLSpectatorI just received the latest Dentistry Today.
2007 Dental Buyers Guide Issue.In it there are a number lasers mentioned.
Many of them claim to work great on everything.
Many claim various modes of transimission that are better or more suited to their use….for example,
Ultraspeed CO2
-general, surgical, periodontal, endodontic, implant, and aethetic/cosmetic procedures. The “Sapphire Resonator” seems to be what allows this laser to work on everything.Lumix2
-nonsurgical cold laser for biostim only. 40W peak power.several others but I’m tired of typing.
So, my question is, what is true?
and of the things that are not true – why doesn’t the company get in trouble for making claims?Thanks.
dmd92eastSpectatorHow do you detemine if you have the right water and air settings. By the way, I really like this laser. Positive feedback from patients and I use it on just about everything. From cavities to soft tissue to even cleaning off CEREC preps. Pretty cool.
AnonymousSpectatorDave, somewhere on LDF is a thread about this. My recollection is 13-15ml/minute for water although I try to get both air and water low enough where I’m not likely to drown anyone and also not get any ‘brownout’ during prep. If I find the thread I’ll post a link.
AnonymousSpectatorDave, I just tested my versawave and it is between 2-3ml/minute. It was my Waterlase that puts out between 13-15ml/minute. Maybe Glenn can get us the ‘official rate’ 😉
dmd92eastSpectatorThanks, I know the manual whicj I don’t have in front of me right now states I believe 10-15ml’s per minute but don’t quote me. So I sat there with a graduated cylinder and did this. Pretty, pretty, pretty boring and no that easy to get right at it. Then of course my water wasn’t coming out at all so I played with the nob and screwed it all up. Turned out my water bottle needed a little more elbow grease tightening. Well anyway what about air? I see the MD has all this computerized. Is it real important? And are these easily calibrated? How do you check air rate? Soory for these stupid questions but also trying to bring some life back into this forum. I’m a wee bit concerned that it is so dead in here.
Glenn van AsSpectatorDave: My suggestion is to get to either Nasth or LVI for training. That will help. Try to get around 14-18ml per min. If you get too much the patient starts drowning and the cutting is slowed and too little and pain and charring starts to happen.
Hope that helps
Glenn van As
Glenn van AsSpectatorHey Ken: as you know I am using the Velscope and like it alot. Its a challenge to make sure of not getting false positives but it sure does open up some good quetions about oral cancer with patients.
Check out <a href="http://www.velscope.com
Hope” target=”_blank”>http://www.velscope.com
Hope all is well. Alfred Wyatt also has one and loves it.
Cya
Glenn
Nick LuizziSpectatorDave:
If I may add to Glenn’s post. Vacuum size and placement becomes an issue. If the vacuum tip is too close to the tooth, the drawn on fluid flow becomes an issue as does charring and discomfort. Too far away and it becomes a problem with diminished effect from the erbium and plume. This is where the art comes in, and visual learning based on effect become important. You must enter into each proceedure with the idea that you observe the variables. The book will take you only so far. Then throw in the human factors associated with the patient and the fun really starts. I also strongly agree with Glenn, get to LVI or other learning center where you can surround yourself with guys who have tons of experience and can guide your learning curve. It’s worth every penny.
Hope that helps. Nick Luizzi
etienneSpectatorHi Guys
I saw this patient again in November 2006. I was disappointed in the response of the furca lesion. I re-treated the tooth in question with the laser. I also placed a temporary crown.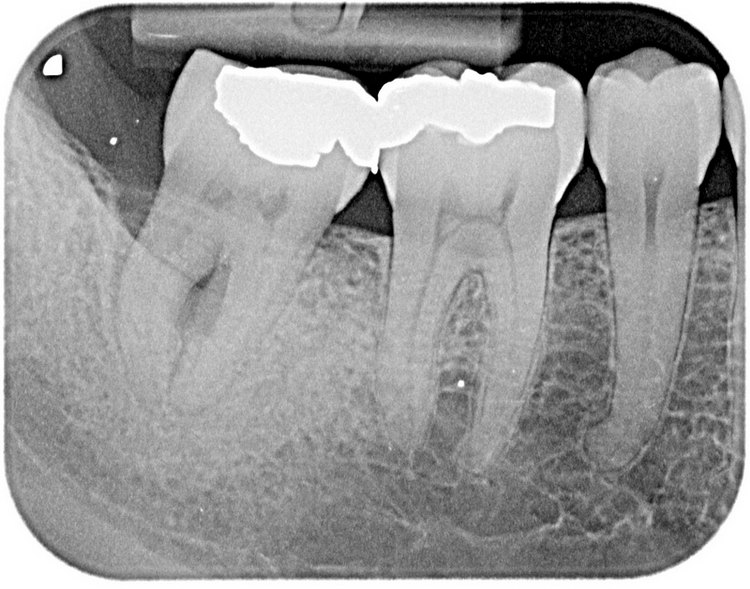
I saw the patient again this month. This is the newest x-ray.

I think it is clear that the distal defect is healing. What is happening to the furca lesion? Healing? Clinically it looks good. No more drainage from the lesion. I did not want to probe yet.
Any thoughts?
Take care
Etienne(Edited by etienne at 2:23 pm on Jan. 21, 2007)
Robert Gregg DDSSpectatorHi Jason,
FRP Nd:YAG dentin etching is much different than FRP Er:YAG dentin etching.
Free running pulsed erbiums tend to leave a smear layer behind.
Free running pulsed neodymiums tend to leave a melted and resolidified layer (aka “reactive dentin”) that is much more resistant to decay and microleakage due to increased bond strengths.
Lots of literature describing these results.
Good question.
Bob
-
AuthorPosts