
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorHi Pat: I think that my errors were caused by the soft tissue tip, not being careful enough with the positioning of the tip when cutting ( I now try to stay parallel to the tooth instead of perpendicular when trimming the tissue away). In the typical case I dont have it now.
The scope is a fun thing and it allows me to actually remove the patient from the equation by focussing 100% of my attention on the operating field. It eliminates the patient who makes faces from interrupting my concentration and I leave this area to my assistants.
The scope is fun , but there is a big learning curve to it.
I havent done many inlay preps with the laser so kudos to you. and there are no laws against using intralig or even intraosseous if the patient is not comfortable.
Good stuff .
Ron nice case, nicely prepped and restored.
Great stuff.
Glenn
SwpmnSpectator[img]https://www.laserdentistryforum.com/attachments/upload/williamsa09.JPG[/img]
Ron/Glenn:
Figured I better flip the maxillary photo and crop out the mandibular teeth or Glenn would get mad!!!!
Just kiddin guys,
Al
SwpmnSpectatorNice cases Glenn and Ron Kaminer.
Thanks for sharing!!!!!
Al
Glenn van AsSpectatorIn the first pic I thought you had patients with palates on the mandible……..
Great photos Al, and your story of how you came to appreciate and use your laser is for me one of the three or four best things from the forum
Others include Rons rise in knowledge and his pursuit of the science and physics behind lasers.
Bob Greggs constant history, science , and physics posts, he has forgotten more laser stuff than I will ever learn.
Mark Colonna proved to me that crown preps were possible with the laser and that you dont need a sundial to time the preps.
IN addition I have really enjoyed the comraderie, pics and education I have received on this little ole site.
I want to wish everyone here a warm , safe , and prosperous new year. May all your dreams come true.
Keep on lazin’
Glenn
Glenn van AsSpectatorHi folks and a best wishes for the upcoming new year.
I am going through some old pics and seeing things that I might think are of interest.
Alot of times we have discussed things with the lasers but there havent been cases shown.
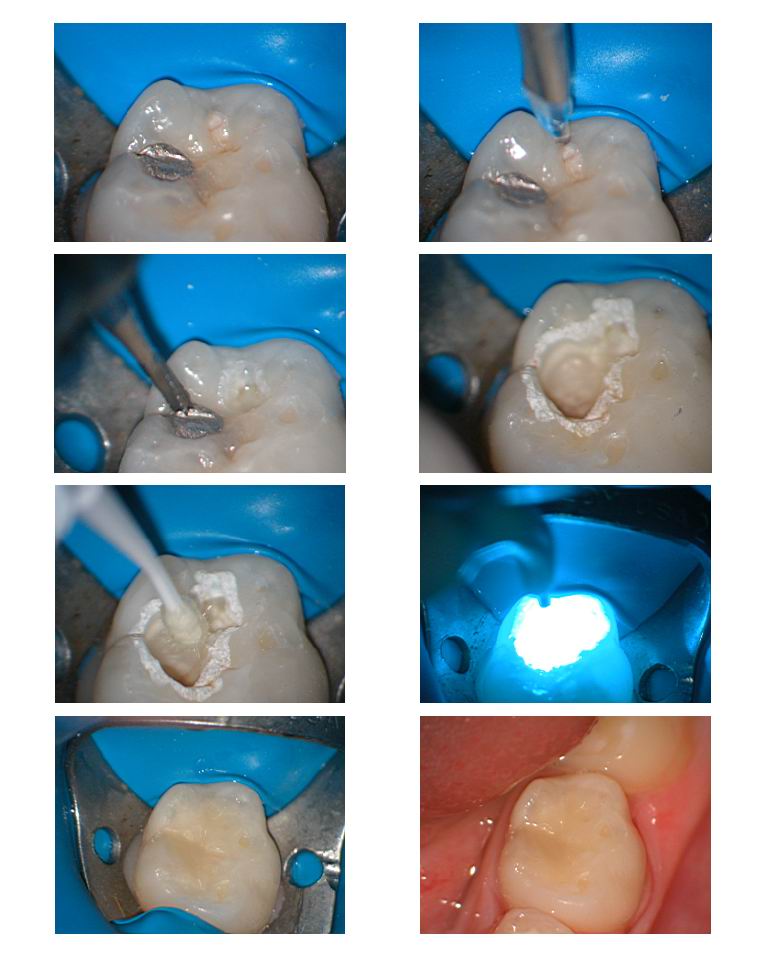
In this case there was new decay on the occlusal of a primary molar that had an occlusal amalgam in it.
Some of you have been anesthetizing the tooth in defocussed mode for 60-90 secs at high wattage (5.5-6w) with lots of water and air and then going to the amalgam.
What I did here was remove the caries first which takes that long and then go after the amalgam with a bur and once removed join the two areas up with the laser.
The laser removes the smear layer and the tooth was bonded for a composite restoration. For those that are new, the argon laser at 488 nm was used for curing.
Hope it helps solidfy once of the concepts we talk about here……….
The laser helps desensitize the tooth and alot of times you can then use a bur for amalgam removal afterwards without sensitivity.
Glenn
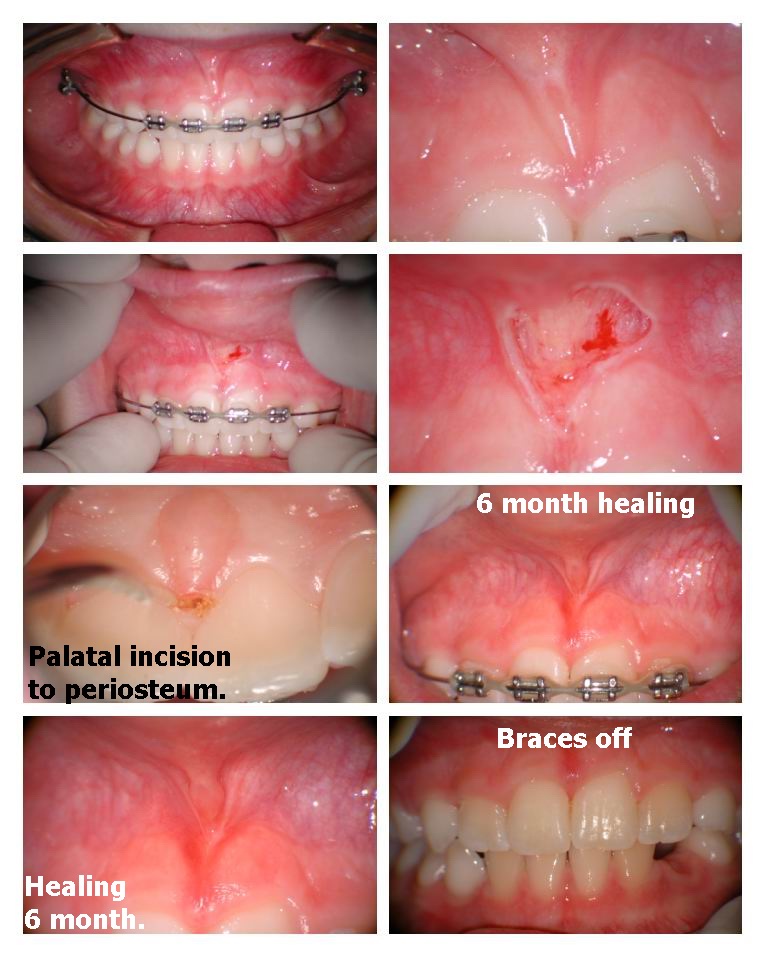
Glenn van AsSpectatorHi folks this frenectomy was done on a 9 year old whom the mom is presently refusing to have orthodontics done but wanted to see how much the frenectomy will help.
Rather than arguing about it , I will do it while telling the parents that the odds are not in favour of it closing.
I then will do the ortho at 11 -12.
The keys with frenectomies is to see if the elastic tissue goes right through to the palatal and if it does you must remove the fibers.
There are two ways. Larry Kotlow uses this technique where he actually goes through the fibers from the facial troughing right through the papilla to the palatal.
I prefer to actually release the fibers on the facial and then make a small incision with the laser soft tissue tip on the palatal right down to the periosteum to release those fibers.
I use anesthetic here although some claim that EMLA is enough. I dont want to do it 2X so I use anesthetic.
One thing you can do is to blow air on the surgical site gently to see if there are still fibers remaining. With the scope I can see if I still have fibers left to remove , but often without the high mag it is tough to tell.
Once you cut through the last fibers is when the bleeding starts, sometimes I have to use the Argon laser or you can use an astrigent solution or pressure. It will often take more time to stop the bleeding than the frenectomy which takes all of 90 secs or so.
Hope this helps………..
the last two photos are of the healing and the patients are generally not taking anything except Advil at times for the first day or two.
Glenn

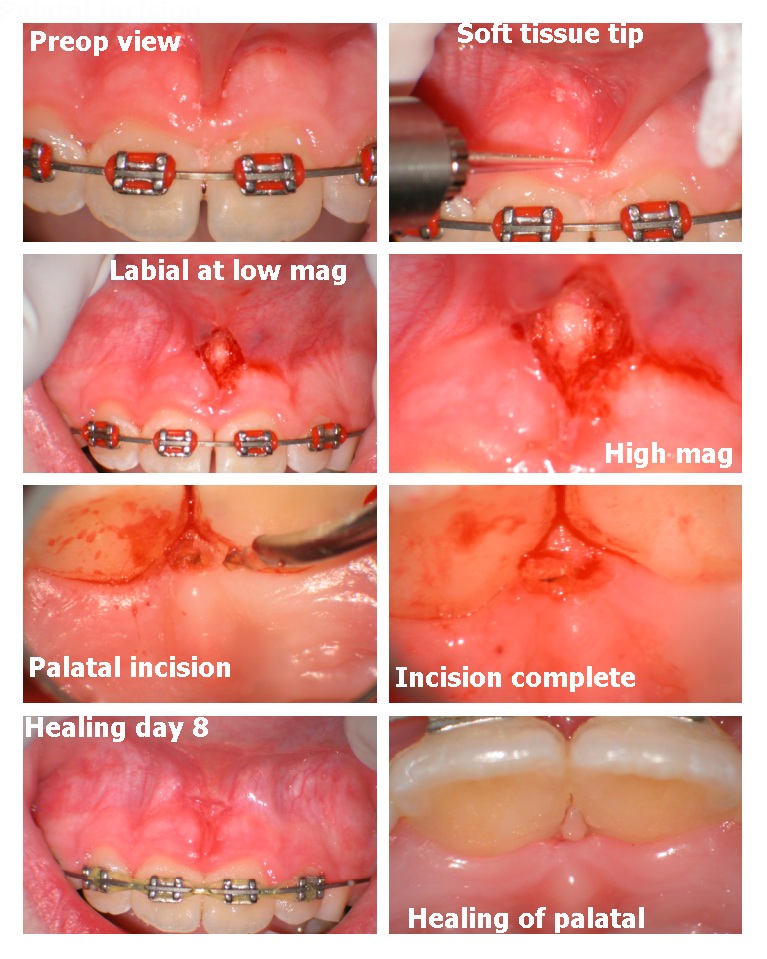
Glenn van AsSpectatorHere is a 2nd Frenectomy done with the method I like of making a small incision on the palatal right down to the periosteum on the palatal. This method was taught to me by Dr. Larry Finkbeiner from Colorado springs who is a periodontist who routinely uses the Argon laser for these.
The healing was uneventful and if I can find another case I will post it for you of the healing.
The settings are typically 30Hz and 80-120 mj (2.4-3.6watts) without water for the soft tissue with the pointed soft tissue tip which cuts a little cleaner and faster than a regular tip.
Magnification helps you see the fibers and prevents you from having to redo the frenectomy.
Hope this helps stimulate some debate.
These are easy and are 200 dollars per frenum so if you are interested in doing these then at least you have seen some photos.
I typically give them a bottle of Chlorhexidine and tell them to swab it with Q tips 2 times per day for 6 days and then see them on the 6th day.
I also advise them, no hot sauces, and to expect only a little discomfort, often it seems like it starts on the 3rd day once the nerve fibers start regenerating. Advil works fine for that. The laser dulls the nerve fibers (obtunds) and it really isnt too sore usually for the first couple of days and then sometimes mild discomfort for a day or two come day 3.
Hope you like it.
Glenn

Glenn van AsSpectatoroops the file didnt upload.
Here it is.
Glenn
Glenn van AsSpectatorHere is a third one that shows the healing at 8 days. Again you can see the slight bleeding when cutting the tissue on the labial.
I used a curved tip in the palate for easier positioning (its tough to get the straight soft tissue tip in the palate on a little kid).
The healing photos are at 8 days.
Glenn
whitertthSpectatorGlenn, Great stuff…. I have done a few but I am still somewhat hesitant for fear of anatomical structures…but with your pix,I am ready to jump in and do more….Happy New Year
SwpmnSpectatorRon:
I began with the Waterlase in May 2001 and the trunk fiber blew about two weeks later. The second trunk fiber blew this summer while a Biolase technician was repairing my laser.
The technician told me that water left in the delivery system and corn starch from powdered gloves are enemies of the Waterlase. He said that I should purge all water from the delivery system after each usage. Also suggested keeping the laser out of sunlight when not in use. I have full wall windows in ops and he said this can heat up any water which remains in the system.
Personally, I theorize that contact with metal substrates like amalgam, PFM crown margins and old bases where you see “sparking” can damage the trunk fiber. We know for sure that this damages the sapphire tips.
Also, I stopped moving the Waterlase between my two main ops. We have now a “crown prep/laser/radiosurge” room and use the other op for simpler procedures and when it is not practical to use the laser, e.g. seat crown, amalgam “patch” of PFM crown margin on 95 yo female.
Al
SwpmnSpectatorGlenn:
As usual, nice cases!
Is that the “handpiece”-like delivery attachment for your Continuum you are using in these photos? Also, what are the dimensions of the tapered tip you are using?
What is the Continuum website so that I may learn more about your laser?
Al
SwpmnSpectatorGlenn:
Cool case, use the laser first to remove caries and desensitize the tooth then use bur to remove amalgam.
What bonding system are you using to place your composites? I notice that you always etch with phosphoric after your laser preps. Are you placing a flowable for first layer?
Since April of this year, I have been prepping carious virgin teeth only with the laser then placing Clearfil SE Bond with no phosphoric acid etch. I place a flowable composite first on my posteriors, currently using DE-MARK from Cosmedent.
Patients are cycling through recalls, reporting virtually no sensitivity and composites look great.
Al
2thlaserSpectatorMan you guys, I have been off vacationing over the holidays, and here you are all teaching without me! I feel left out! Just kidding. Great stuff. I get back to work on Thursday, and have tons to share when I get back. I hope everyone had a great holiday season. Excellent cases!
Mark
2thlaserSpectatorRon,
What did you notice while cutting the first prep? Then, what did you do between that one and the next? There are many reasons you can blow a fiber. I can help you there depending on what you observed. I haven’t (knock on wood) blown anything in a very long time. There are certain things I ALWAYS look for before starting procedures, and also on how you and/or your staff maintain the laser in between appointments, and inbetween days of use. That is why I wanted to start this particular thread/section. I KNOW it is part of the learning curve that we can change for everyone.
Mark -
AuthorPosts