
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorHi Allen: no this is the pen type delivery system. WIth the scope its hard to see around the back of the handpiece so I use surgical length burs alot to get the back of the handpiece out of the way of the scopes viewpoint.
Conbios web site (they are conbio now and not Continuum after selling of their industrial and custom made laser section.)
The old site is still there at
http://www.conbio.com/mainswf.html
Gosh the tip is very narrow at the tip and about 1 cm long.
I dont know the actual dimensions…….I apologize for that maybe I can post it when I find out.
Glenn
Glenn van AsSpectatorAllen: your questions are always so astute.
Thanks for the kind words by the way.
I still dont feel comfortable using SE bond because the local bonding guru told me about the possible failures of 6th and 7th generation (no etch) bonding systems which he termed as fine on dentin , not fine on enamel.
I think the laser etch probably is enough but old things die hard for me.
I use a 5th generation bonding agent , Prime and Bond NT (one bottle bond) after I etch.
I am not in the majority anymore when I look at polls. There are alot of people doing exactly what you are doing.
Don Coluzzi whom I really respect is doing exactly what you are doing with Clearfill SE bond.
He loves it too.
I often use flowables in the base like tetric flow and then hybrids like Tetric Ceram. Some times in kids I will use Dyract Flow and Dyract.
Thanks for the compliments. ALot of the tiny preps are only possible to treat with the flowables.
I thought the pics were good on that one so that is why I posted it.
Happy New Years to you All
Glenn
Glenn van AsSpectatorHi mark: We are going on without Ya but I am just passing the time til you get back and start showing of veneers, full mouth reconstructions, endo , perio and a little bit of other disciplines using the laser!!
Take care have a safe and happy new years Mark.
Glenn
AnonymousSpectatorAlan, Mark,
We purge the system every night .
The unit is moved about 3 ft max at the beginning of the day.
I had finished prepping number 3 and stopped to talk to the patient about the next tooth we were going to restore. I had the handpiece in my hand the whole time.
When I stepped on the peddle to start up again there was water spray and air and a very faint pop corn sound , probably not even 1/10 the noise I usually hear at 5.25W
I changed tips , same thing. Next changed handpieces, same thing.
Next I activated the laser w/o water or air on 1.0W and moved it over my gloved hand and felt no heat. That’s when I guessed it must be the trunk fiber.Any suggestions or recommendations are appreciated,
PatricioSpectatorAl and group,
I have been wondering when I prep with the laser and leave a roughened surface what additional value the etching adds. So far I am using clearfil SE but am trying the new stuff I think it is called Simple?? which is a little different. I notice Glenn is really roughing up the occlusal margin and it looks like maybe a bevel has resulted. What are others doing?
Pat
SwpmnSpectatorGlenn:
Thanks for your input on bonding after laser preps.
Read my post on Dental Town under “Feeling Great About my Waterlase”. It’s actually a serious post about my experience with soft tissue surgery but I threw in some humor to try and break the ice.
Al
SwpmnSpectatorPat:
I think Glenn posted on Dental Town research results which show about 90% bonding of laser only enamel etch compared to phosphoric acid. When you also etch laser treated enamel with phosphoric the bonding strength is increased by about 30% over phosphoric etch alone. Personally I think when we get above 20 MPa bonding strength the differences are clinically insignificant.
You are using John Kanca’s Simplicity product, right? How is it working for you so far? I’m quite interested in the product.
Here, I use the Waterlase to strongly etch the axial occlusal margins on a posterior tooth but try not to create a bevel. I’m concerned that composite on beveled posterior occlusal margins may fracture over time.
Al
SwpmnSpectatorHey Mark!
I’m the one who started the Maintenance thread! Look under General Erbium Discussion(page 2)/Usage Maintenance Tips.
Just kidding with you man, doesn’t matter who started what!
Please post what you have learned about maintaining your laser so that we can all learn.
Al
Glenn van AsSpectatorHi folks: here is a case where I wanted to band a lower 2nd molar and was patiently waiting for the tooth to erupt.
Finally, impatient, I used the Argon laser which will cause less bleeding than the erbium. A diode or NdYag could also be used to help it out.
1 Watt continous wave with some anesthetic and then the tissue was reflected enough to get the band on.
Electrosurg can work but causes 5X the energy dissapation to surrounding tissue.
Glenn

Glenn van AsSpectatorHi folks : heres hoping a great start for you all in 2003 both professionally with your lasers and personally with families and friends and relatives.
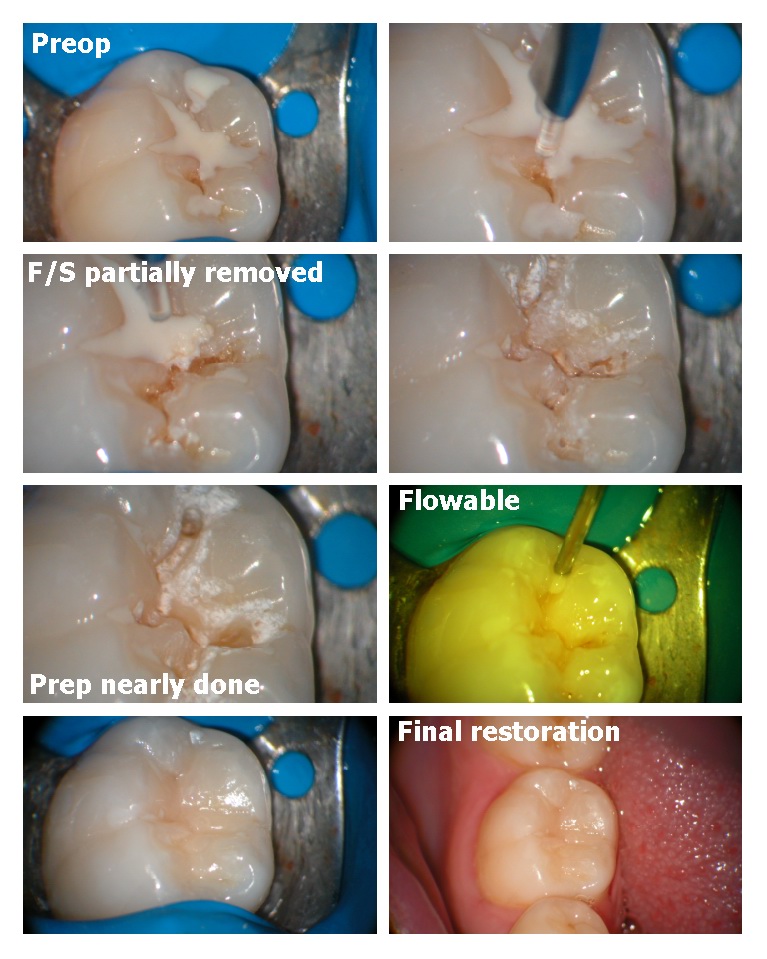
I just thought that it would be nice to show a failing F/S (fissure sealant) case.
I dont often put F/S in teeth anymore. Back in the mid 80s when I was in dental school we were taught if it wasnt sticky, just stained to seal it.
Not a great idea in my mind as the diagnodent show all these stained grooves are above 25-30 except in smokers. The fluoride in the toothpastes makes the enamel harder but its still decalcified and the FS doesnt stick to them.
I dont think that etching the surface and placing a sealant seals these teeth at all. In fact I think that it just acts as a food trap.
With the scope I often see at high mag shadows under the sealants when looking at them or a piece will come off and I will remove the rest and lots of times there is decay under them.
Occlusals are the hardest teeth to prep with the laser so often I will do a hybrid technique using the laser initially to anesthetize a bit, then a series of small high speed burs ( 1/4, 1/8th or 1/16th burs from Brassler) to widen the preps and remove some decay and then the laser again to remove the smear layer.
If the decay is into dentin ( it often is) the patient feels the burs if you dont use the laser sometimes.
THe laser removes the F/S very very fast, and in addition if you dont follow the grooves with the laser tip but go back and forth over the grooves perpendicular to them you get a much better result ( you flatten the cuspal slopes ) and then can get into the grooves faster.
Here is a microdental case, I usually fill them with flowables.
Happy New Year to you all , man 80+ members now.
Hey Ron it sure would be nice to have a member page with a profile, where you practice , what type of practice you have, what lasers you use , when you graduated and a photo so we could see who is a member here.
Great to put a face to the name……….
All the best.
Glenn
PatricioSpectatorI was thinking when looking at Glenn’s pictures how much easier it is to fill and finish the occlusal aspects of a restoration. The materials can be more exactly feathered to the tooth margins and excess all composite removed. This makes the final finishing steps fewer, quicker, easier and much more pleasant for the patient. Glenn is the flowable holding up well? I still use regular composite except in the very small pit type preps. What are others doing/
Pat
PatricioSpectatorAl,
Thanks for your comments. Yes I am using the Simplicity. So far I have had to learn to clean the prep with alcohol without flooding the patient’s mouth. The sponges privided hold way to much but I have it down now. The self etch liquid is clear and a little more difficult to see on the bracket table vs the Clearfil. The resin is much thiner and only requires 5 to 8 seconds prior to curing so that is a plus. The idea was to develop a thinner resin interface so I would say this is a success. There should be virtually no pooling of the resin. I have been using the Rembrandt Saphire light for curing with complete success. In most cases we use 3 seconds for each application. This makes for a smooth flowing procedure without 20 second delays.
Pat
Glenn van AsSpectatorHi Patricio: THe pics are so much easier to take then having a digital camera that you have to grab each time.
Mind you , there is the learning curve of the scope to get over but the pics are easy to get.
I have forgotten how much more difficult it is to work without the magnification, but it really helps you limit how much composite you place, the finishing process.
I still maintain that alot of white lines are due to inadequate bond or etch which leads to failures not caused by anything else than a lack of vision.My preps now are very conservative, (1/8th or 1/16th round burs do that for you) and the only thing I can get in there is flowables which for me are almost like a fissure sealant but more highly filled with resin.
They are holding up but remember you have to be able to see them first (loupes or some magnification) then after diagnosing the lesions , adequate magnification allows you to be far more conservative in the preps.
John West found that his accesses done under the scope were 67% smaller than those done without the scope. Its the same principal we use in Oral Surgery with flaps which are for visibility (and sometimes access).
Now because of the scopes I dont have to widen up the preps unnecessarily to get enough light in to see whether all the decay is gone.
We diagnose earlier, we treat earlier and I think more conservatively.
I know that some dont agree with this mentality but it came to me only when I started using the scope and saw what I was missing.
Finally, one last thing, my new years resolution is to complete my trifecta this year with a third scope for the hygiene room (because often when I diagnose one restoration to do at a recall appointment, I notice there is another one to do in the same area when I get the patient back with the scope).
i also am aiming for a diode to improve my soft tissue capabilities ( sorry Bob I know it should be an Nd:Yag but I am working it out in trade for lectures etc. with Continuum …..paying full price too.)
Glenn
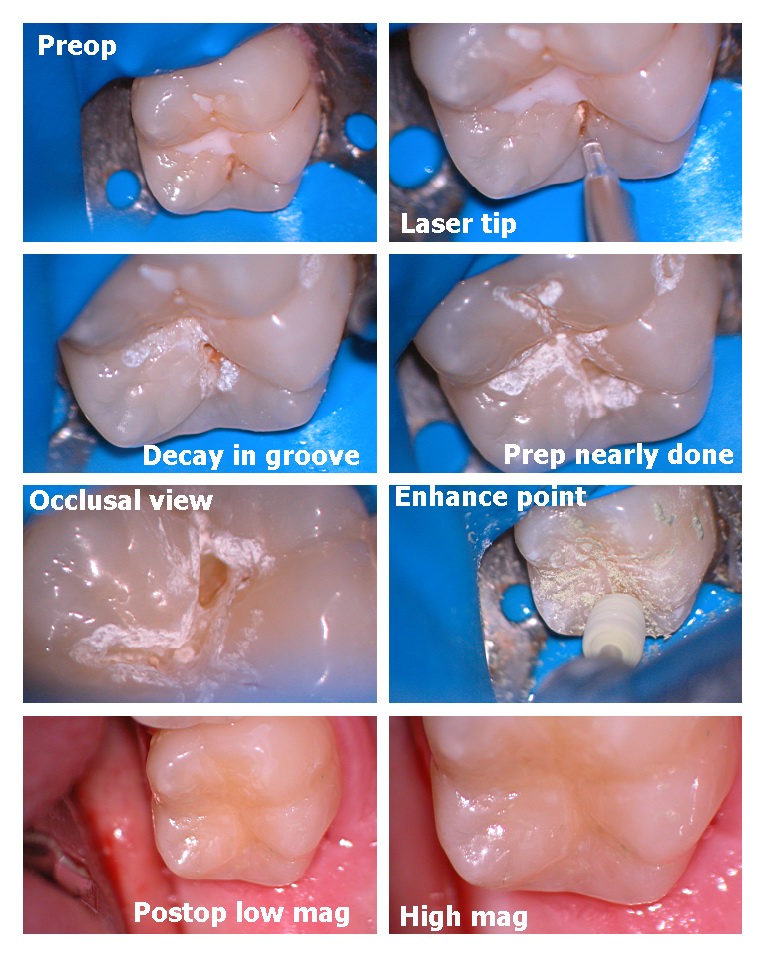
Glenn van AsSpectatorHere is another microdental prep where no decay was visible under the sealant when I got it off and the decay was localized to the distal pit.
Into dentin it was 3mm deep.
Flowable as well placed. I have not noticed them breaking down in the 2+ years I have been doing them this way but others may beg to differ.
I would love some feedback from Ron and others as to the value of the photos and also the layout that I am using.
i am trying to keep the size down so that I dont use up all Rons space and hope that this is suitable for all parties involved.
Glenn
I can also post it to another site Ron, like Sendpix if it is a problem.
PatricioSpectatorHi group,
I lost two trunks during the first six months and then 6 months off. I lost a fiber about two weeks ago when water began to drip from the unit end of the trunk. The hand piece still worked but water everywhere. For the first two failures which were like Ron’s I have no idea what happened but it is possible we have since stopped some activities which were burning out the morrors etc. as Al suggests. Careful maintenance seems to be improtant but I am not yet sure what the keys to success are. My assistant follows the directions and I feel pretty dependent upon her ideal care. I do not do anything personally to maintain the equipment. Should I?What did I learn Al? I had the two fiber trunks repaired at no cost to me and I now have two spares in the office so I can be back in business in 15 minutes. I called for a repair number and a new fiber arrived in my office as a replacement so now I am back to three trunks in the office. Being in the eastern time zone it took a day and one half for the new fiber to arrive. With only one fiber in the office you will be greatly inconvenienced or your patients will be grumbling about the SHOT and the DRILL while you wait for your new fiber.
Pat -
AuthorPosts