
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorOh I feel so bad that I didnt get there this year. How many people came…….what were the best lectures . What did you like seeing there the most.
I wish I could have come and is it worth while to get the CDrom or DVD or whatever is produced of the whole meeting.
Glenn
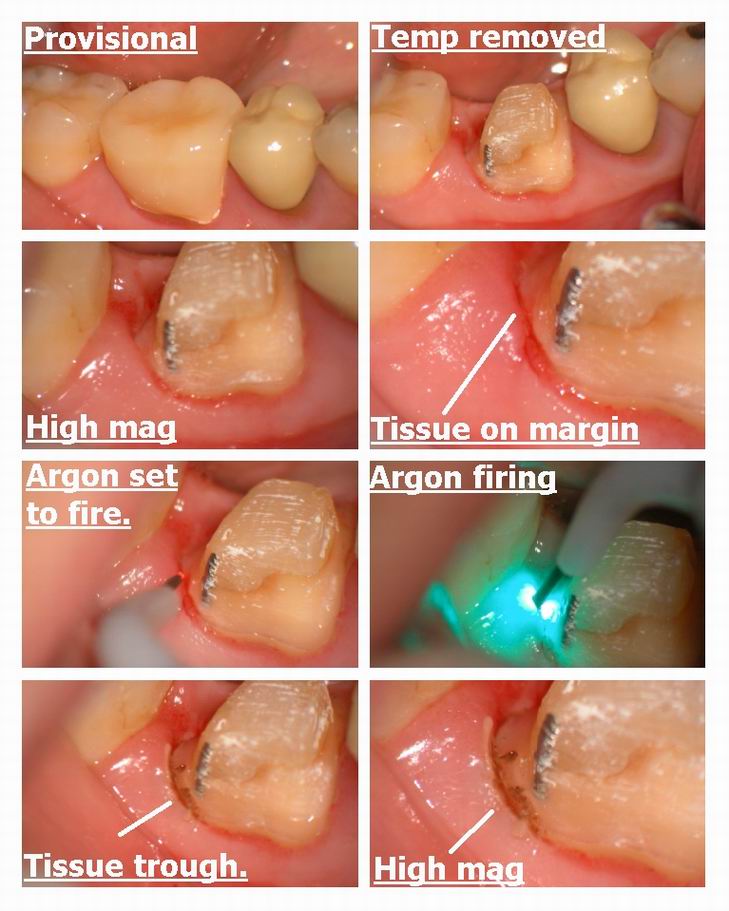
Glenn van AsSpectatorHi folks: Here is a simple thing that shows how a soft tissue laser can be used to help with a crown cementation.
At high mag once I got the provisional crown off I noticed that the tissue had slumped onto the margin on the distobuccal of the tooth. I had anesthetized the patient previously so I used the Argon laser to reflect the tissue away.
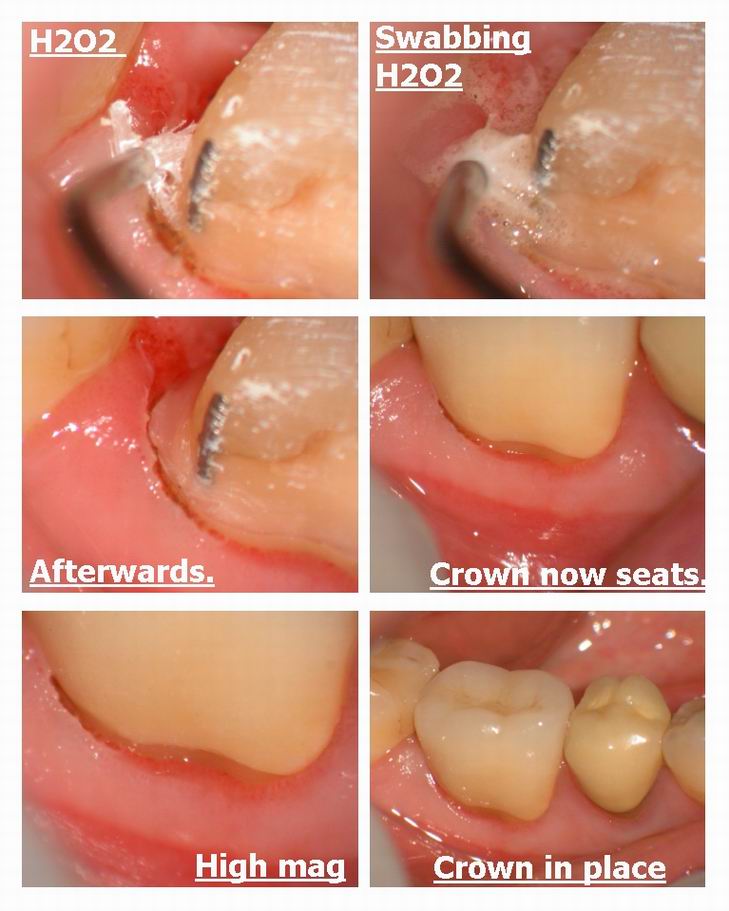
It leaves some tags so often I will then use hydrogen peroxide in the Ultradent syringe with the mop thinga me jingy to swab the margin and remove the tissue tags.
I think that it became very easy to seat the crown after trimming the tissue back and the magnification showed me that the tissue was still on the margin. Argon is cool as it is the only visible wavlength and I still get a kick out of the photos that we get using the wavelength with the scope.
SImple case……….note how easy it is to see the margin on the buccal.
Here is part one of this case which was a failing onlay.
Used the erbium to retain the core with pins……..ya ya I know some of you hate the pins!!
Cya
Glenn………
Here is the link to part one of this case. It is the 4th post on the thread.
http://www.rwebstudio.com/cgi-bin/ikonboard/topic.cgi?forum=29&topic=36
Glenn van AsSpectatorDid you have a good trip?
Glenn
Glenn van AsSpectatorHi folks: Here is a case I did today for a nice patient of mine who wanted to improve on his smile. Wanted to remove the stained restorations and in addition wanted to uncrowd the teeth and even out the gingival heights (he is in the dental field).
I used the Argon laser at 0.9 watts Continuous to sculpt the anterior four maxillary incisors and then prepped the teeth and then took an impression and temporized.
Two canines are veneers to match the premolars which have crowns and the four incisors are full coverage crowns.
I rounded out the tissue and got a nice result with the temps I thought.
TIme will tell. PS you can do this with an Nd yag, diode or an Argon………the diode and Nd yag the tissue might stay a little better and not recede on the facial.
Glenn
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of Taylor pg 1_p1.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of Taylor pg 1_p2.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of Taylor pg 1_p3.JPG[/img]
lasersmiledrSpectatorAfter trying to reinvent the wheel with the Pulsemaster, I became a Periolase user.
First, thanks to Bob and Del for being pioneers in the field. The difference in tissue response, effectiveness etc is undescribable.
Much hype is out there on other wavelengths etc. Sound science should be the basis for making a decision for those sitting on the fence. Millennium is the only company that I know of who fully back their product, do the research and provide a standard protocol in order to get consistant results.
Who else out there is putting their money where their mouth is with a 6 month full money back guarantee? Dispite this, I know of NO returns! That should speak for itself.
If a practitioner cannot make money with this machine in his or her office (cause their is a lot of perio out there as well as a long list of other documented uses) he or she needs to find another profession .
The best test beyond the clinical aspect which is extremely significant, is the verbal response from the patients themselves. I am still waiting for my first negative response.
Thanks Bob and Del for making me a hero for my patients and giving me great joy in a profession I love. And thanks to the organizer of this fine forum for productive discussion of the technology available today!
Todd McCracken, D.D.S.,M.A.L.D.
2thlaserSpectatorNice case Glenn,
I am off to Copenhagen and Frankfurt tomorrow, so I probably won’t post much, unless I get a high speed internet connection. I have a few cases I did this past week to post. Glenn, I appreciated your response in the other thread. I will be careful not to go overboard with not seeing my family, etc. Thanks for your concern. I hope to be in touch while gone, but if not, see you all next Monday.
Mark
lasersmiledrSpectatorThe advice found here is excellent! Do your research, realize the limitations of each wavelength, pulseduration, instrument etc.
I find it misleading though as mentioned earlier, this forum location is for NdYAG lasers. Both the Biolase and Continuum are Er lasers and forum discussion for them is best suited elsewhere.
Todd McCracken, D.D.S.,M.A.L.D.
Robert Gregg DDSSpectatorGlenn–
We really missed you being there.
I enjoyed Jeff’s presentation, of course, but he really did an excellent job, dealt wiith the pressure well, deflected the barbs thrust at him, and he really did confront Peter and dragged him to see the histology. Peter looked impressed after explaining the study.
Also, the lecture presentation on Polarized Optical Coerence Tomography (P-OCT) by Daniel Fried of UCSF was very interesting. It uses a handpiece and light source to emitt near IR light to detect caries and loss of perio structures (eventually) with detailed resolution. More precise than DIFOTI or Diagnodent. It is technology in its infancy, but has a lot of promise. Technology is licensed to Lantis Laser, a private company Craig Gimbel formed some years ago.
I spent a fair amount of time talking with Tom Haney about stuff. We had some good talks. He was re-elected manufacturer rep to the ALD board. I tried out the HCB erbium. Cuts well in all the right ways. 220 mj/p and 30 hz was interesting. 210 to 240 usec pulse duration, depending on setting. Couldn’t find anyone at Biolase that knew the PD of the Waterlase. I think it is 140 usec. Tom thinks it is more like 100

DEKA laser from Italy was new to the scene. Pretty mock-up boxes, lots of claims, lots of boasting, no specifics, no FDA, evasive answers from sales rep Chris Justen. Wouldn’t give details on laser parameters. Showed mock-ups for Fr Nd:YAG, CO2, Er:YAG. I’m not holding my breath. He was off-putting to many. Like Bryan Pope said, “He’s gonna come here to the US and learn us ignorant folk all ’bout lasers.”
It was amusing to see the YSGG and Opus Dent advocates present their different perspectives on endo research. I let you fill in the missing pieces….I’ll fill you in when you come down to CDA.
Bob
lasersmiledrSpectatorHi Ron!
Great question! I have experience with the Diolase ST. The functional capablilities of each of these devices are different. I have tried several similar cases in the past. I did note as Bob and Rod mentioned earlier, occlusion is definately key in good perio therapy as well as splinting and removable occlusal splints
Due to the wavelength and absorption characteristics of the diode lasers, lateral damage is a significant issue. Often the very tissues that could form new bone and attachment, are burned with the intensity of Diode laser hence, the attachment desired is not achievable.
To this date, I have not seen a paper that outlines a logical protocol with repeatable results. Although this would be advantagous to the manufacturers to prove and provide this information, I do not see anyone pursuing this project.
I would be very interested to see the long term results on this case. I have a few myself that I don’t mind sharing. Several of these I later retreated with the periolase after the marginal results achieved with the Diode. I did find that wavelength and pulse duration is extremely significant in the outcome in such cases.
I also noted that while crown lengthing with the diode worked quite well, I did not have control of healing as well and if used in the anterior region, often led to an undesirable margin exposure. The NdYAG allows for much more control in the esthetic zone and I now do all crown lengthing procedures (specifically soft tissue) at the same time of preparation. With proper use, I have yet to have an undesirable result and far superior hemostatis than Diode or Er.
Again, high peak power, with much shorter pulse duration with this specific wavelength lend to greater control of tissues and hemostatis.
Best wishes in your search for more answers!
Todd McCracken, D.D.S.,M.A.L.D. 😉
mtweiserSpectatorAnyone have a source for good quality brochures on the use of lasers in treatment of perio and/or hard tissue?
SwpmnSpectatorBob:
The PD(pulse duration) on my Biolase Waterlase is listed as:
140-150 microseconds.
Frequency is fixed at 20 Hz. Pulse energy up to 300 milliJoules.
Speaking of CDA(California Dental Association) in Anaheim April 24-27, I’m going and would like to personally meet the friends I’ve made on Ron’s Forum.
Who else is going to the Spring CDA Session?
Al
AnonymousSpectatorDon’t know about quality but the Academy of Laser Dentistry has some members can order.
BTW, Welcome to the forum!
March 12, 2003 at 3:45 am in reply to: low level laser therapy for pulpitis and healing of oral sur #10678
Robert GreggParticipantHi Jeff,
“Bob, Why would’t you use a wider pulse width when coagulating an extraction site?”
That’s the neat thing about having choices in our devices, we can choose the settings that match our comfort zone.
With wider pulse widths, one has to be very careful not to over-warm the bone. So the “shorter” at 150 usec has sufficient coag capabilities for most extraction sites.
But you are absolutely right about the the long pulse at 635 being a quick coagulator, and one I might also use in a hemophiliac or Coumadin patient.
Remember too, Jeff, you have 4 years experience under your belt, and I want Ron’s learning curve to be a gentle slope, not a “hockey stick”.
QUOTEPulse Width is… time of the pulse?Yes, it is also known as:
1. pulse time
2. pulse duration
3. pulse length
4. pulse shape
5. pulse profile
6. waveform:confused: Sometimes this stuff gets very confusing since there are so many interchangable words to say the same thing.:confused:
250 versus 650 (635) is about 3 x’s shorter in pulse time/duration. That is the time the pulse is ON before shutting OFF and firing again. At 20 Hz (50,000 usec in 20 pulses/sec). Ask Del to do the math! It’s right.
250 usec ON = 49,750 usec OFF (repeats until 20 pulses have fired)
650 usec ON = 49,350 usec OFF
So the refractory tissue cooling OFF time is not changed much at all.
What has changed is EXPOSURE TIME of the tissue during the ON portion of the pulse, that can be varied by a factor of 1.5 x’s to 6.5 x’s for the Periolase MVP-7. Or from 150 usec to 635 for the Periolase I, by a factor of 4.2 x’s. Either way 635 or 650 will coagulate quickly without burning or charring.
QUOTEand the purpose of the increased pulse width-deeper penetration?Yeah, pretty much. Deeper, wider, and to envelope large capillaries with the pulse shape. But now we’re getting in too deep! It’s a longer exposure time to the tissues like the shutter of a camera controls the “burn” of the film. Short shutter durations are good for action shots. Long shutter durations are good for low light conditions. Too much light and we OVER EXPOSE the film. We don’t want to do that with patients’ tissue, so we employ long pulse durations when they are called for.
I hope that makes sense.
Bob
whitertthSpectatorHad a great time in st maarten….8th time down there..kinda like home away from home…trying to get my dental liscence there now and if i succeed i will open an office laser equipped…we shall see…..Regards
ps Mark can u pack me away with you….
Glenn van AsSpectatorHi Allen: I will be there for the meeting working with Continuum (Hoya Con Bio and Global) make sure you come by and say hi
Bob , what an EXCELLENT synopsis. I can read between the lines. I think that certain laser companies are concerned alot about science and the ALD always has a loyal crew of followers for those lasers. It seems that the Millenium is falling into that fold.
On an aside , I am sorry I missed the ALD , but the buzz that was created by the scopes at the Pacific Dental Meeting here in Vancouver was fun to see.
Dr. Jeff Coil (head of endo at UBC) and myself did a lecture + hands on workshop and it went really well and created alot of interest. 2 years ago I had 4 people for the hands on . This year we had 34 I think.
The lecture had double the number of attendees and John Wests scope + endo course was sold out.
He had a full day lecture and he emphasized the role of the microscope and basically said you can do the things I am doing without one.
Great buzz at the booth and Vancouver being my home town and me working hard to legitimize the usage of the scope for ALL procedures it was heartwarming to see.
I missed meeting everyone but we will have a laugh or two at the CDA in April.
Cya
Thanks for the synopsis.
Glenn
-
AuthorPosts