
Forum Replies Created
-
AuthorPosts
-
SwpmnSpectatorASI:
We are approaching two years with the Biolase Waterlase Erbium. If operating properly, the unit is excellent for treating HARD oral tissues such as enamel, dentin, carious dentin and osseous structures. When we have required service, Biolase has provided rapid response and we have an outstanding service technician here in Florida.
However, there are two major issues I will present:
1) Failure of Trunk Fiber Delivery System and Laser Components
We are now using our fourth trunk fiber delivery system – the cable or hose which attaches to the laser handpiece. When the trunk fiber blows you cannot use the laser. Just beyond our one year warranty period, the flashlamp, pumping chamber and laser rod failed. We had to purchase an extended service contract for 񘴘 per year to maintain our laser.
2) Handpiece
The Waterlase utilizes a “handpiece” to deliver Erbium energy which looks just like a high-speed turbine. Problem is, the “handpiece” angle is set at 90 degrees, which is incorrect for dental treatment and unlike modern high speed handpieces. Other problem is the “handpiece” head is large and blocks your vision if you are only using an overhead operatory light. Since Erbium treatment can only be applied by direct vision(not “feel” as when we use our turbine handpieces), this is a significant factor. I have been able to reduce this problem by combining magnification loupes with a headlamp which I use to directly illuminate the treatment field.
Al
greg holmSpectatorThanks to all for their posts.
This is a somewhat off subject question. What about using the delight or waterlase to remove some of those ‘age’ or ‘sun’ spots we seem to get the older we are? (This is not a question for tx of pts but of myself)?
Another question closer to topic. What is your relative fee for tx of apthous or herpes lesions?
Greg
drpippinSpectatorThanks, Jeff. This is from the Lumenis web site:
February 19, 2003
LumenisTM Ltd. (NASDAQ: LUME) today announced financial results for the fourth quarter and year ended December 31, 2002. The Company reported revenues of ๟.4 million for the quarter, compared to 贄.8 million in the fourth quarter of 2001. The net loss in the fourth quarter of 2002 was ื.7 million, or ũ.07 per diluted share. The loss includes non-recurring charges of ร.8 million principally for asset write-downs and litigation reserves. In the fourth quarter of 2001, the Company reported a net loss of ū.9 million or $.11 per diluted share.
For the year 2002, net revenues were 跼.5 million and the net loss was ฼.1 million compared to revenues of 跛.2 million and a net loss of 贱.9 million in 2001.
I have concerns whether or not a company losing this much money will continue to support its product. The dental divison accounts for only 3% of total sales. It could be the first to be cut.
Glenn van AsSpectatorHi Bill: I agree but Ray Tang and Bob Gregg know alot about the trials and tribulations of these companies and often will post insights as to what they see.
Lasers are a tough business to make money, lots of cash goes into R and D and in addition there is alot of cash spent marketing . Biolase is starting to make some money but boy did they ever pour it out in the beginning and many questioned whether the return would be there for them.
Hopefully Lumenis and Opus are on the same pathway because if one laser company folds it sets everyone back a step. People assume all laser companies are on the verge of bankruptcy.
If anyone is going to the Hinman next week , check out Hoya ConBios new booth. I gather its quite a nice one and I will be giving a couple 15-20 minute lectures there on Thursday morning and Friday afternoon.
all the best
Glenn
BenchwmerSpectatorMore info on the Opus Duo Erbium delivery system:
The delivery system is a hollow wave guide with an attached swivel handpiece ( 2 styles are interchangable a 90 degree or a straight tip, on these handpieces inserts are from 200-1000 micron saphire tips).
The wave guide could be 4-6 inches longer for less positioning of the unit.
I work using loupes with an attached fiber optic light source.
 [img]Jeff
[img]Jeff
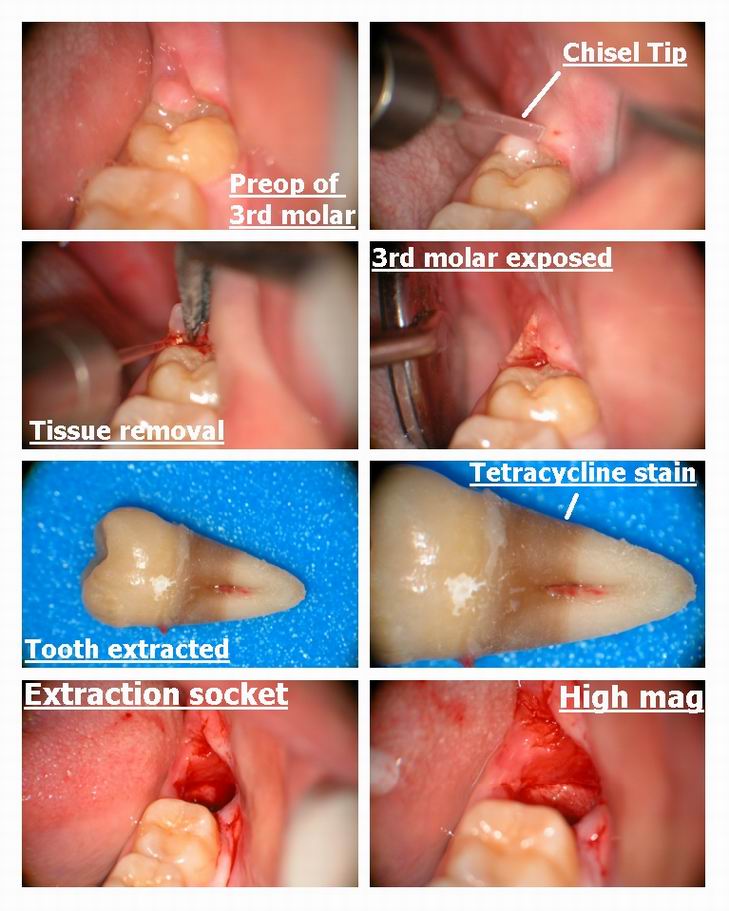
Glenn van AsSpectatorHi folks: Happy Saturday to you all! Here is a case I did yesterday for a nice lady who was suffering from pericoronitis for a lower third molar.
We used the erbium laser to incise and release the tissue and then used it to remove a small piece of tisse on the DL that may have been annoying to her tongue.
I used the unique chisel tip to cut the tissue, without water at 30 Hz and 80-100 mj. Not that much bleeding either.
I could have used a scalpel but there would have been more bleeding.
She was a tetracycline user for a while for acne around 14 or so…..you can see it in the roots.
Have a great weekend…….
Glenn
BenchwmerSpectatorResults
Where did my case go?
Sorry(Edited by Benchwmer at 9:13 pm on Mar. 15, 2003)
toddhryanSpectatorHowdy all!
My first post to this site. I was at the ALD and have been researching lasers for about 6 months now. I first started the laser search thinking that I was going to buy a hard tissue laser. But …. after as much learning as I felt I needed to make an informed decision I bought a Nd:YAG from Millennium and their excellent support staff of Bob Gregg, Del McCarthy, and Rusty. I believe they are the ONLY company that TEACHES their purchasers HOW to use their new lasers. I am looking forward to my training and the use of this great technology.Jeff Cranska did a great presentation and anyone with an open mind at the ALD conferance would have had a lot of questions about this technique of laser periodontal therapy™ and its tremendous results.
The ALD conferance for me as a newbie was very good as I took the standard proficiency class and exam and was absorbing as much info as possible. I quickly learned that I had to sort through the bull_ _ _ _ .
Overall the conferance was well run and well attended. The best presentation I saw was at the hospitality suite hosted by Millennium Dental Technologies. Dr. Bob Gregg had a wonderful power point presentation on their Nd:YAG laser and some of their results. I keep absorbing like a sponge about lasers and THIS site is tremendous and a HUGE thank you to Ron Schalter for setting it up.
I hope to pay for my laser soon so I can start to branch out into other laser dentisry in my office. Thanks all for sharing your knowledge.
Todd Ryan
Hillsdale, MI
toddhryandds@email.com
BenchwmerSpectatorHey Todd, you found the Board.
You’ll be happy with you decision to start w/ a Nd:YAG.
Perio will pay for the Laser, then you have the laser to do all the things daily to make dentistry easier and more predictable.
Keep in touch.
Jeff
rhenkelddsSpectatorI am a new Waterlase user, and have been trying just about any procedure that I can read about and implement in my office. When doing a laser crown lengthening, is there any issues with leaving a negative boney architecture interproximally when doing this with the laser. Traditonal surgery(flap and ostectomy) suggest blending all the bone contours so no depressions are evident. From what I have seen, from other laser users, is that a more conservative laser crown lengthening is much more selective in nature and does not require as much bone or soft tissue removal.
Is it considered acceptable to use a G6 tip in the col area,remove the tissue and two mm of bone and then call it a day, or should we reflect a flap and use the laser to remove and contour bone and then replace the tissue.
AnonymousSpectatorHi all,
Dr. Fried has registered for the forum at my invitation after some of our discussions regarding hydrokinetics and the role water plays in ablation. Dr. Fried is a Phd. from University of California, San Francisco. (see abstract in General Erbium/Hydrokinetics thread)
Those who attended the ALD meeting in Fla. were blown away by his presentation on Coherent (?)Optical Tomography which gives a 3 dimensional ‘ice cube’ image of teeth.
I’m looking forward to his participation .
Welcome Dr. Fried!
lagunabbSpectatorTerrific! Welcome.
I have a question for Dr. Fried on Nd:YAGs posted on the soft tissue laser thread.
lagunabbSpectatorDr Fried:
I asked Bob Gregg the question below to assess the difference between theory and application for Nd:YAGs. Can you please comment specifically on the way that Nd:YAGs are being used and how potential problems are avoided in practice. Some manufacturers such as Lares suggest that Nd:YAGs can be safely used to selectively remove pigmented caries.
Bob,
I talked to someone last week that held your system in high regard. In reviewing (again for the 4th time) the Fried et al’s paper “Mechanism of Water Augmentation” Laser in Surgery and Medicine 31 pp 189-190 (2002), they wrote:quote:
Extensive damage to the mechanical intergrity of the bovine block and thermal damage to the underlying dentin was observed after irradiation with the free running Ho:YAG laser at 2.1 um (see Figure 5) even with a layer of water applied to the surface. Laser light at 2.1 um is only weakly absorbed by water. Therefore, it is able to penetrate through that water layer without the transfer of much energy and through the outer 1-2 mm layer of enamel where it is absorbed by the dentin resulting in thermal damage. Monte Carlo simulations of light deposition in teeth followed by calculation of subsequent temperature rise have predicted localized thermal damage at the dentin-enamel junction (DEJ) during Nd:YAG (1.064 um) irradiation without ablation of the outer enamel. Localized subsurface damage was visible at the DEJ after Ho:YAG irradiation. At higher incident fluence, thermal stresses generated at the DEJ produced large fractures transverse to the path of laser irradiation resulting in the destruction of the bovine enamel block. This result exemplifies the danger of irradiating teeth with free-running Nd:YAG and Ho:YAG laser pulses — even with entensive water spray.
Their Figure 5 shows SEM’s of subsurface damage to dentin at 70 J/cm2 and extensive thermally induced DEJ fractures at 150 J/cm2.I would appreciate any thoughts or comments about this experiment and their interpretations. Thanks.
SwpmnSpectatorThat’s pretty cool.
The chisel tip is coming straight off your attachment to the fiber, correct? In other words it is parallel to the direction of the fiber?
Are there advantages/disadvantages to using the Er: YAG vs. your Argon laser in this situation?
Photo of the stained root is quite interesting. I used tetracycline at about the same age and wonder if mine had those bands. Apparently your patient ceased treatment as the apical portions were formed.
Just out of curiosity, do you happen to have a pre-op radiograph of that tooth in digital format?
Al
SwpmnSpectatorGlenn:
Nice case and excellent use of lasers to access the margins!!!!!
I’m not being critical at all but just want to offer some some thoughts on my experience with core buildups:
1) Contrary to my training, I placed my last pin in the Fall of 1989. With modern dentin bonding agents, particulary the new self etch primers combined with Erbium laser treatment, I bond my cores with absolutely no fear of them becoming dislodged during prep, impression or removal of provisional crown.
2) In past years I placed many cores with a composite which was radiolucent. Some were long-term treatment plans and I would take radiographs of these patients which had acrylic provisional crowns/bridges. When I viewed these radiographs, I couldn’t differentiate the core from the tooth and couldn’t tell if I had left caries.
Also, probably because I wasn’t using magnification, through long term recalls I found that I had placed some final crowns on radiolucent buildup margins. Difficult to tell whether recurrent caries at the margin or just a radiolucent composite buildup so I stopped using radiolucent core materials and now only use radiopaque light cured posterior composites.
Al
-
AuthorPosts