
Forum Replies Created
-
AuthorPosts
-
Robert GreggParticipantDang Pat, you’re deep!
I’m with you all the way on this as well. I like your parallel thinking.
Lasers have made me appreciate my clinical practice in ways that others find very……different.:confused:
Bob
SwpmnSpectatorEmeril is the man! My favorite quote, “I don’t think people should be eating to live, I think people should live to eat!”.
Realistic, “wet-gloved” expectation for most of us to prep un-anesthetized patients with an Erbium laser: 50%.
That’s about what I’ve found after almost two years. The “Defocused Technique” where you bathe the tooth for 60-90 seconds at high settings helps somewhat. Others may strongly disagree with me.
Couple of examples:
This morning, preparation of #11 disto-lingual Class III composite with laser. Theoretically, this should be an easy tooth to anesthetize, right? Clinical requirement to complete restoration: 3 carpules of anesthetic.
This afternoon, Class V preps on #21 and 28. Theoretically, one would expect these preps to be sensitive and more difficult to place without local anesthesia. None was required.
My point is, just like today, placement of restorations using the laser without anesthesia is unpredictable. Many factors are involved and I believe the most important factor is the patient. Personally I believe the majority of patients who can tolerate laser composite preps are probably the same patients you could prep unanesthetized with a high speed handpiece.
Al
Glenn van AsSpectatorAbsolutely poetic in its knowledge………..I can give you no greater compliment Bob.
Your posts on soft tissue and gingival curettage are worth the price of admission………….wait a minute its free here………ok let me rephrase that.
Your knowledge about soft tissue periodontal curettage is current, complete, and sparkled with enough science and research to make it always a great read.
Thanks again……..god I wish i had the money for an NDYAG.
Grin
Glenn
Glenn van AsSpectatorHi Allen: I did that decay around the amalgam last week and here are three pics of my fiber window that I shot today. There are air holes and water holes but no damage to the window there.
Glenn
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of DSCN5044.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of DSCN5045.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of DSCN5042.JPG[/img]
Glenn van AsSpectatorHI guys: great posts. I did several things to help me with patients and sensitivity.
First I acknowledge that most patients will feel something. This pain in most cases is tolerable but it is there.
I ask them if they feel something typically a cold sensation or discomfort to raise one finger (not their middle one I tell the adults) and on a scale of 1-5 for the pain tell me how bad it is. If they get to 4 or 5 then I lower the settings, desensitize more or evaluate how much further I have to go.
I had to numb someone up today after I finished the first occlusal on a 15 year old male the second one I had to numb up.
In another kid he told me he didnt want the laser……it took too long he told me (he had it before around a year ago). This was the first time anyone had complained about time.
In closing another thing I do is use the rubber dam with alot of patients even without anesthetic except one touch topical from Hagar and I often will tell the patient that if they can stand the clamp on the tooth that they wont need a shot ……..I phrase it like that or I say the needle.
They often take a sigh afterwards knowing that for them the worst is over and they will be ok.
I can tell you that the second time around most laser patients are a breeze, its the newbies that require alot of TLC and explanation.
In closing the scope and watching the procedure really helps as they know how much longer they have to go and disassociate themselves from the process when they are watching.
Just some ideas but in closing Pat , Dr. Don Coluzzi told me years ago to put the anesthetic away, as we are taught in dentistry that whenever the patient feels anything when we numb them that we need more anesthetic and most patients will feel something but verbal skillls confidence in the technology , knowing a few tricks of the trade all help to increase the success rate.
Glenn
Glenn van AsSpectatorHi Jeff: congrats on your purchase and tell us more about the Opus when you have a chance.
I think Lumenis who owns Opus among many lasers is having a bit of a tough time these days , so do make sure that you get everything you paid for and do have service on it if you need it.
I have played with the machine and know that it works. Let me know more about how you like it and post some pics if you can.
I went to your web site last night. Nice clean site and interesting reads.
All the best and congrats on your erbium purchase.
Glenn
Glenn van AsSpectatorAlmost there Mark……..I have a little gift for you today if I get a chance to post it under the erbium section . Look for it in an hour or so.
Glenn
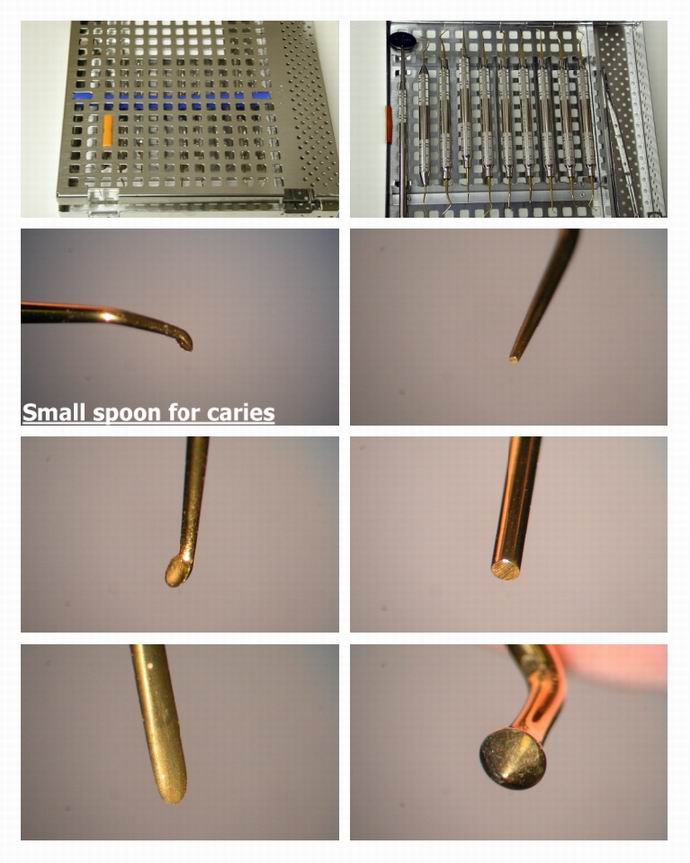
Glenn van AsSpectatorHi folks: Well I received my special instruments (paid full list price I might add) from Mark Colonna today and used them on a non laser prep.
Kid said the laser took to long last time!!
I prepped with some microprep burs from Brassler and then had a little bit of decay left which I removed with the smallest spoon.
There are 11 instruments all double handled except for the mirror and cotton pliers.
There are 3 sizes of spoons, some small pluggers and some felt instruments and some fossa/ cusp formers.
I like the feel of the instruments and quickly took some photos……..they arent the best but they are ok.
Here is the case and the photos ….hope you like them and support Mark by ordering a set or two…….
How is that for support when I dont get a dime.
glenn
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of Preps layout pg 1_p1.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of Preps layout pg 1_p2.JPG[/img]
Nuno FerreiraSpectatorGlen. Since im been using turtle procedures by Dr Chen, i can manage much better my pt confort but everytime they refer some i take some minutes with defocus tips and circle motion in cervical (both V and L) but also near the last tip locacion patient felt something…and Glen the result as been very good. In this case afther all this procedures i reach pulp chamber and we dont need to look to know it because patient NOW as some…so a placed some topics in there for about 60 seg. and then you can do everything , i use NiTi to determinate canals lenght with apex finder.
I know that some treatments take some time…and this time is more or less with de experience and trainning of all of us. BUT GOD IT FELT SO LOVELY WHEN WE CAN DO IT… AND PATIENT LEAVE HAPPY.
Sorry about my English, soon i will place some pics and other cases, LOVE u ALL im a lonely Portuguese waterlase user im very glad to have found all of u.
BenchwmerSpectatorGlen,
I am a Microdentistry advocate. I’ve been using air abrasion for tooth preparation, preparation for sealants, composite repairs, abfract restorations, etc for almost 10 years. When the caries spirals and spreads at the DEJ, AA is not the instrument of choice for caries removal. Air abraded dentin allows some caries excavation w/ #2 round bur in slow speed or a spoon without discomfort.
I purchased the OpusDuoE to use with AA on occlussal caries. AA is quicker in removing enamel, gaining access to caries in the dentin, then I use the laser for analgesia, to remove the carious dentin and bacterial decontamination. I am surprised how I still need that #2 round bur.
Bonding is accomplished with the 6th or 7th generation self-etching DBA, I like Kulzer’s new I-Bond, single bottle technology, w/ Gluma. No seperate acid step or rinsing. No liners (for me since 1995) No patient sensitivity.
I have the Nd:YAG for MicroPerio Surgery, now I’m using a Erbium for hard tissue microdentistry.
If I ever get back to work ( 2 feet of snow has Maryland closed down) I’ll photograph some cases.
I’m still on the way up the learning curve w/ this laser.
I will have questions. Thanks.
Glenn van AsSpectatorJeff, you and I share many of the same beliefs and I look forward to your posts.
I still too maintain the need for th #2 burs.
I have an assortment of microprep burs now from different sources that include ultrasonics, small diamonds (#1 and 1/4 burs) and also some carbide burs from Brassler (003,004 and 005 ) which are 1/16th, 1/8th and 1/4th round.
The microscope and the diagnodent help alot in seeing these incipient lesions but it has been my experience that in adult Class 1 and 2s that the laser is not the ideal instrument for opening up the enamel. AA or small burs work better.
If the decay tracks laterally , the laser is not that good for widening preps.
If the decay is really mushy it also isnt easy getting it out.
Hope that helps
Glenn
2thlaserSpectatorOk, time for me to “chime in”. I agree with all of you, pre-verbal desensitization is the first step in successful anesthesia with the laser. Like Glenn, I ALWAYS tell them they WILL feel something. Mostly a “cold” sensation, like ice cream freeze on their tooth. Now, as many of you have heard me say, I haven’t had to anesthetize anyone since last Feb. for any routine procedures, except about 50/50 on Endo procedures. My staff really is well taught in their verbal skills to work this through prior to my walking into the operatory. Next, I re-enforce those ideas while I set up my laser and it’s settings, right in front of them. Mostly, I try to use humor, it really is the “ice breaker”. Patience, and persistance is the rule here. IF you are patient enough, and persistant, you will gain greater control over your technique, and the anesthetic effect will get better and better, I promise. DON”T RUSH INTO THE DENTIN! You will be surprised how easy it will become. I always say, if you were to wait for the anesthetic, then drill, you have that 10 min to kill. After 2 min of defocused “anethesia” with the laser, and I “chat” with the patient the whole time, guiding them through what I am doing, it is so much faster than the old methods. Another thing, don’t let your assistant keep asking, “are you ok?” every time the patient “seems” to feel something. Let the patient tell YOU. Just remind them once or twice, no need to implant into their grey matter that it SHOULD hurt. That is the old style of dentistry. We laser users are still amazed that we DON’T hurt people, at least I am. Even after a year! And what a year it’s been. I have more to share, but I got to get my son to school, and me to the office. More to come tonight!
My best to ALL of you, you all are wonderful to share in this forum together, thanks!
Mark
Robert Gregg DDSSpectatorGlenn,
Thanks for the compliment…I think…..:confused:
You don’t need to worry about the $$ for our Fr Nd:YAG. The patented LPT procedure pays for the laser in 12 patients (24 Canadian);)
Bob
SwpmnSpectatorThat’s pretty cool, Glenn. So the tip just pops right into the end of the fiber?
How much did that burned out tip set you back?
Al
2thlaserSpectatorAlso Glenn, is there a mirror to “foul” in your handpiece? As we have a mirror in ours to deflect the laser energy out the tip at a 90 degree angle. Here is a picture of a “fouled” tip.

You can also see the angle, like a bur in a high speeds angle, the tip exits from the handpiece. Disadvantage, mirror, advantage, feels like regular dental handpiece, which alot of people like. I personally would love to have both a straight and the conventional laser handpiece (hopefully Biolase reads this board huh?)
Mark -
AuthorPosts