
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorHi Pat……..the scope is not for everyone but I tell you it sets you apart like lasers from the guy down the street and it sure does allow me to do better work than I could before.
I use the scope for new patient exams, we leave the TV on and allow the patient to follow along as we read of what work exists and what needs to be done.
Often I will use Morita retractors and place them in and allow me to look with both photographic and small mirrors.
I had a lady today whom I finally convinced her to have a crown done on a fractured tooth. Every tooth has fillings that are five surface big.
I placed the crown (she was watching on TV) and then she asked me about her front teeth. Well every tooth in the maxillary anterior has restorations that are huge.
She is coming in all excited as she wants to go ahead and do the crowns up there.
WEird how things are but the scope and the attached video create more work than I can handle and lately its mostly cosmetic.
IN addition I rarely have to explain what I am doing , and patients never question me anymore if I find two restorations, have a pulp exposure find a crack etc.
Its alot less stressful for me now.
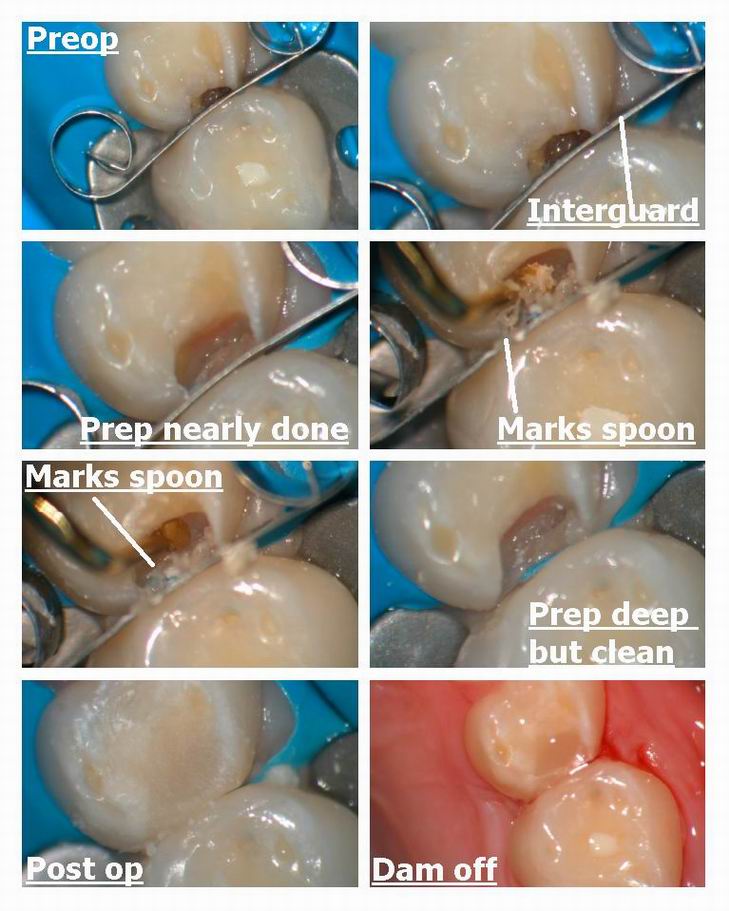
Gotta go finish a lecture but here is a little gal we had today (daughter of one of my hygienists who is a single mom ) and the little girl had quite a large DO on the first primary molar (upper left)
All done without anesthetic…..nearly hit the pulp.
Used Marks great little spoons that are sharp as heck and really nice. Mark I mean that, they are excellent.
Glenn
SwpmnSpectatorNice case. Yesterday I placed a buccal pit #19 on 8 yo male and occlusal on his 10 yo brother #30 without local. I used the “defocused” technique and seemed to help. Glad it worked out since mother is a former oral surgery assistant!
The occlusal on #30 was very similar to your deciduous tooth case.
Glenn, in picture 4(second row, right hand column), is that a “bubble” of water on the proximal end of your laser tip? I haven’t seen that and found the photo intriguing.
Al
Glenn van AsSpectatorHi Allen ……….man you are perceptive. This is the 400 micron tip. There is alot of teflon coating on it and that is indeed a bubble of water.
I was half way through the prep I guess I wanted to show the laser was cutting.
Thanks for pointing that out. ITs things like this that magnification show you when you dont see them with your own eyes.
All the best Allen……..you sure are astute. I missed that.
Glenn
Janet CenturySpectatorBelow is an email I received from someone reading my website. Has anyone heard of this type of treatment? Perhaps she means desensitizing for the pulpitis thing. I was told by my rep that I could use the laser to help clot after extractions (ie coumadin patients) but I cannot think of any further “treatments”. I wanted any input before I email her back.
Thanks so much
Janet“Hello. I was reading your website and noticed that you have treated cold sores and canker sores with lasers. Do you also practice low level laser therapy for pulpitis and healing of oral surgery sites? I have been going to Wisconsin for this kind of laser treatment and am looking for something closer to home. Thank you.”
March 6, 2003 at 4:47 pm in reply to: low level laser therapy for pulpitis and healing of oral sur #10670
lagunabbSpectator<a href="http://www.karna-ddscomfordent.com/LLLT-2.htm
No” target=”_blank”>http://www.karna-ddscomfordent.com/LLLT-2.htm
No FDA approvals yet for the applications shown by Dr. Karna.
March 6, 2003 at 4:52 pm in reply to: low level laser therapy for pulpitis and healing of oral sur #10675
Janet CenturySpectatorThank you very much. It is an interesting concept, but I’d like to know if anyone here has tried this.
Thanks
Janet
2thlaserSpectatorGlenn, Again, fabulous work. I HAVE been AWOL! I have been in Chicago, and off the net for about a week. I am leaving to lecture in Scandinavia and Germany next week, then off to London in April, SO, that being said, it has been difficult to get online. I took some photos today of a case I did, and will try to get it online when I can. I looked at scopes in Chicago, and will test drive one very soon! USE MAGNIFICATION, it’s awsome! Listen to Glenn everyone, he knows what he is talking about, because HE IS DOING IT! DAILY! Thanks for sharing so much Glenn, you are a credit to dentistry!
Sincerely,
AWOL….Mark
greg holmSpectatorPat. There is a major difference in the ‘look’ of the prep after ‘cleaned’ by aa. The ‘schmutz’ or I suppose the smear layer is visibly ‘cleaned of any residue or debris which will be apparent after aa use. They look pristine. I probably would not do a fill or cr prep now without aa ‘cleansing’, the difference is that obvious. I have no scientific data, just personal observation.
Greg
wiemsSpectatorSo I did my book training for my ng YAG laser (Lares Pocket Pro 8 watt), but I have yet to have my hands-on training. I have used my laser for tissue troughing around a couple of crowns, and and it seems obvious when the treatment is done for these situations. Today, i used the laser to do some sulcular debridement on my dental assistant (a couple of 4-5 mm areas), and I really didn’t know when I was finished or not. Any advice?
Also, I notice that the filament tip collects melted tissue residue, and it doesn’t necessarily come off easily. It seems to collect on the sides of the filament, and the tip seems clear. is this OK, or do I need to clean or re-cleave the tip during the treatment?
I also noticed that there was melted tissue residue on the teeth that I troughed for crown impressions. it was sticky black stuff that I had to remove with a scaler, which got things bleeding. I finally just pulled out the Viscostat to close the deal so i could get an impression. Is this normal to have this residue, and any advice for removing it easily?
Lots of questions, any feedback would be appreciated! Andy
dkimmelSpectatorGlen, I know it takes an effort to post. Thanks. I can see that the scope is a big plus. Do you have one room that you work out of or do you have more then one scope?
David
Glenn van AsSpectatorHi David : I have two scopes (started with one).
You can buy one set of optics and with some of the scopes you can change them from room to room if you purchase an arm and fiberoptic for each room you work in.
If you rooms are narrow you can swing the scope from room to room like an xray and have one scope servicing two rooms.
I bought a scope and mounted it in the ceiling solid in one room and then a few years later bought my second scope.
Mark , I had a long talk with Keith Bateman here in Vancouver today at the Pacific Dental Meeting , had a few laughs , talked alot and your name came up.
Make sure you test drive the different scopes that you are testing, and you know what I use but if you are gonna buy another brand that is ok but make sure you talk to me first privately. I can save you some grief.
I thank you for the kind words on scopes. I am glad to see you travelling so much and enjoying yourself. Make sure they pay you well for it, that your family gets to go sometimes as well. You can get stroked and stoked doing this each and every weekend and guess what……..one day your family isnt there anymore.
Look at all the biggies……it happens to their family life.
Make sure you find balance…….I know the best thing I did was let my wife help me decide where to lecture and where not to go. I have given up the opportunity to lecture in Egypt and Caracas because it just didnt feel right from a safety standpoint. It would have been fun to go but not at the sake of safety.
Thanks for the kind thoughts Mark and it really was funny sitting down with Keith today after all that we both have been through.
You gain a better understanding of the man, I still may not agree with some of the things he believes in but we can agree to disagree on certain items.
Oh ya he grinned about the WCLI and my lecturing there and mentioned that he might like me to come and speak about scopes with lasers (without getting into brand names ) and he might be intersted if certain people (like you , Rod and others ) thought it would be interesting to hear that topic.
ALl the best guys and thanks again.
This is a great group.
Glenn
2thlaserSpectatorGreg,
If you are using a laser to prep, you do not need to use aa to “remove the smear layer”. The laser does that, period! I believe, if you saw a SEM of the tooth after laser preparation, you wouldn’t WANT to touch it with anything other than your bonding agents. I know that Stu Rosenburg, and Kim Kutsch, who are very much into aa, AND lasers, agree with me on this issue. Are you using a laser to prep? When I check your profile, it says you don’t have a laser. Just wondering. If not, yes, I agree, use aa after the drill. Good observation.
Sincerely,
Mark
AnonymousSpectatorAndy,
I’m not a nd:YAG user (yet-will be in about 2 months, thanks Bob G.) but from my experience with a diode, black is either char (which you don’t want) or remnants of the carbon paper used to ‘activate ‘ the tip.
Any chance of posting pictures? I’m sure someone could tell you exactly what it is then.
greg holmSpectatorMark. No, I don’t currently own a laser. But, I am convinced that sometime in the not so distant future I will have a delight or waterlase. I have seen and demo’d the waterlase but want to check out the delight too. I really appreciate Ron’s site here and all of the posters information. Being able to have access to the experiences of people like you, Glen are extremely helpful when considering such an expensive purchase and new technology.
Yes, the preps I was referring to are those done with a conventional high speed handpiece.
GregMarch 9, 2003 at 11:53 pm in reply to: low level laser therapy for pulpitis and healing of oral sur #10671
BenchwmerSpectatorThere are many uses of lasers the limit is in the imagination of the dentist. FDA limits the laser’s company’s advertising claims, but does not tell dentists how to practice dentistry. You practice under your state’s practice act. You will, however be held to standards for misappropriate and harmful use as they affect your patients, as you would a scalpel or handpiece.
Your laser training, educational certification, experience, CE units, etc come into play.
Also what laser do you use? Type of wavelength, power setting, pulse widths, Type of tip, pulsed or continuous wave matter. One laser does not do all.
I use one of my lasers for decontamination and coagulation after every extraction. No calls at home for post-ext bleeding, No dry sockets in 3 years.
Low energy applications can be used post Endo to promote periapical healing, healing post soft tissue surgery, after tramautic accidents, etc, etc. New uses everyday.
I just got back from the Academy of Laser Dentisry Conference. Thirteen dentists recieved the Academy’s Advanced Profiency Certificaion, over 50 the Standard Certification. In workshops and presentations I learned another dozen uses and taught others some of my techniques. It’s a continuous learning cycle. -
AuthorPosts