
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorGreat stuff Jets fan. In general if I use anesthetic I will at least use the bur for alot of the procedure.
Its just my way .
Those patients who need anesthtetic often are not fun patients at the best of times ( at least in my office) and we want to get them in and out of the office as quickly as possible.
Glenn
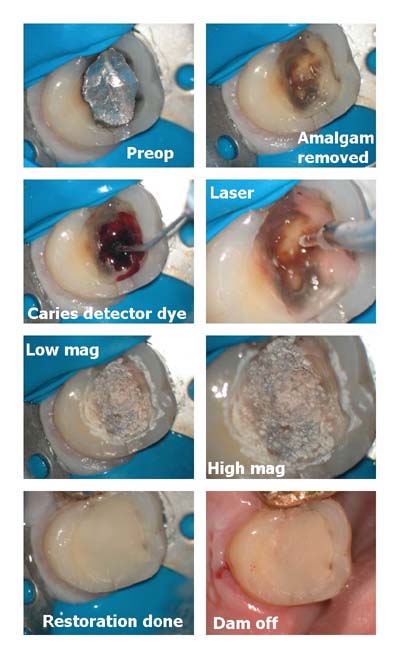
Glenn van AsSpectatorHi guys: I think that Rons photography is awesome.
Next I would have used a round bur on the buccal as I think that is still decay.
The rest looks awesome.
I hate leaving decay behind and like my continued use of etch in teeth I may be following behind at the ripe ol age of 41.
I am interested to see what others do. i hate leaving decay behind.
Just my .02 cents worth.
Glenn
2thlaserSpectatorHi guys,
I agree Glenn, I try not to leave decay behind, BUT, I don’t use a handpiece that often either. Another suggestion would be to, (which is what I do if I see the above stain after lasering), use a small #4 mini spoon excavator in the lesion, not only to test if its stain, because if it IS stain, the sharp spoon won’t remove anything. BUT if it is decay, you WILL remove dentinal debris, then go back with the laser on a very low setting for just a second to “resterilize, and etch” the dentin surface, and then place your agents and bond.
Here is a picture of one of the microdental spoons I have developed just for this procedure I do.Mark
2thlaserSpectatorI will try to upload the image again, Ron, Help? I don’t know why it won’t upload properly, it’s 89K, so it’s small enough! I renamed it, maybe that will help?
Mark

2thlaserSpectatorSorry about the size of the previous photo, Ron is working on helping this out. I can use a laser pretty good, but it looks like digital reimaging need some work huh?, or shall I say DUH?:confused:
Mark
Glenn van AsSpectatorHi Mark: I think some of your viewpoints may change when you get the scope and see the leathery texture at 10-16X mag of the stain. If you test this stain with caries detector gel it will discolor.
Having said that there is argument as to whether it is necessary to take all the decay out. I hate leaving decay period. If it is a pulp exposure , I want to know.
I also think putting a solid restoration on unsolid foundations (caries) makes the restoration under occlusal forces more prone to leakage.
I think with the laser that it is very easy to leave decay behind because under high mag it is tough to get all the decay out at different angles because the laser is only endcutting.
Mark, keep this post and see if your approach changes (mine did) when you start using the scope routinely. I found often that I would etch a tooth and see that leathery appearance of decay……..shoot. Go back in with a small round bur (when I thought I was done) and then the laser , then re-etch etc.
Glenn
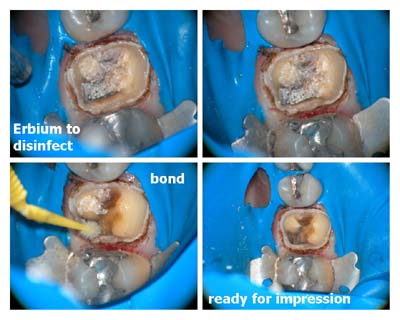
Glenn van AsSpectatorHere is a simple thing I do to make sure the stain is stain under amalgams when I am doing a crown prep is to use the erbium quickly to disinfect and then put gluma or just bond on the tooth to decrease sensitivity and to disinfect the tooth.
Are any of you doing anything similar.
Glenn
AnonymousSpectatorGlenn,
I do something similar but use Hurriseal instead.
At a CE course a few years back they said Gluma, since it is gluteraldehyde based, actually desensitizes by ‘fixing’ some of the pulpal tissue after it makes its way thru the dentinal tubes.
I looked a little for PubMed articles and it seems some say Gluma seals about the same as everything else and some indicate greater pulpal effect than other desensitizers.
2thlaserSpectatorI do the same thing Glenn. I routinely sterilize using the erbium laser after crown prepping with the highspeed/and diamonds. I feel that not only the reduced sensitivity, BUT the increased retention, very low wattages used BTW. You guys are so ahead of the curve, I love it!
Mark
AnonymousSpectatorHi All,
If you can keep you images to 400 pixels in width it will allow the forums to keep their ‘shape’Thanks
2thlaserSpectatorGlenn,
I believe you! Coming from the wisdom of you and your scope/laser, I can’t wait to get into the learning curve you have already completed. I am sure as I get into more magnification, I will see things much differently. I also know, my goal, to use less rotatry instrumentation, will still be my goal, but to that end, how will the “view” from the scope change my “sight”? That will be the challenge for me. I embrace the challenge, and to that end, the teaching I hope to get from you as I get into the high magnification world of dentistry. Again, thanks for mentoring us all with your wisdom in magnification, and lasers. I know I appreciate it more than anything.
Mark
jetsfanSpectatorcould you be a bit more precise…does very low wattage mean, .25W 0%/0%? Additionally, when it is advised to use wattage in a certain range, how does one decide where to begin. Does it depend on the actual machine and how it is tuned, the patients sensitivity level, the level of “wear” on the tips or all of the above. Tangentially, I was wondering or hoping that Biolase could come up with a device or a meter that will clue us in as to when the tip is in need of replacement.
Glenn van AsSpectatorSheesh that wasnt the one I wanted to upload……….
Here are the pics.
Gosh that was dumb
I will answer the other questions tonight, off to pick up my son.
Glenn
SwpmnSpectatorI tend to agree with Glenn. If the dentin is discolored, I believe caries remains and we should remove the discoloration. Yes, sometimes I get pulps. Most of the time I get lucky with 3M Vitrebond, Clearfil SE Bond and flowable composite.
When I get deep I use a spoon and 95% of the time can still pick away “infected” discolored dentin with a spoon excavator. I don’t use a round bur because I hate the slow speed but go back in with the Erbium until the dentin is either yellow or red. If red, I use the above mentioned capping technique and inform the patient that the tooth may require root canal therapy.
So far, since May 2001, success rate around 90%.
Al
SwpmnSpectatorOk, Glenn, now I understand. First pics posted with the composite were slightly confusing.
In general, I use diamonds in an electric handpiece for gross reduction/amalgam removal on crown preps. The Erbium laser is then used for caries removal, “etching” and “sterilization”. Most of the time time I will then place a crown buildup by bonding a composite with Clearfil SE Bond.
Your idea of using the Erbium for disinfection and then placing Gluma or a bonding agent to decrease sensitivity is excellent.
Al
-
AuthorPosts