
Forum Replies Created
-
AuthorPosts
-
Robert GreggParticipantGlenn,
What I noticed on second look was the fracture line appears to extend to and under the buccal cusp tip.
Was that obvious from another view not photographed? That would explain the symtoms the patient describe.
How’s the patient’s tooth and chewing now???
Bob
SwpmnSpectatorThanks Andrew and Glenn.
Andrew, the DELight appears to be a well designed Erbium. I particulary like the small profile handpiece with the curved tips which allow excellent visualization of the preparation.
Al
BenchwmerSpectatorThere was a core build was done w/ bonded composite, that makes it look like more exposed tooth.
I only exposed a mm or so of crown.
Can’t impinge on biologic width.
Jeff
SwpmnSpectatorJeff:
Thank you for sharing your case.
How do you find the hollow wave guide fiber delivery system on the Opus Erbium? Is it flexible and easy to direct the handpiece into the treatment area?
I read some information on the Opus Erbium indicating that it has a variable Pulse Duration. Is the Pulse Duration user-selectable? If not, did Opus provide some sort of chart showing what the PD is at a particular setting?
Also, I was told that Opus has certain tips for their Erbium which are very inexpensive. Have you tried these tips and if so how did you find their ablation efficiency?
Thanks,
Al
SwpmnSpectatorAndrew:
As Glenn says, the PD is listed in the DELight’s accompanying materials as 300 usec. However, I think in a personal conversation I had with Tom Haney at ConBio the PD is around 240 usec(if anyone who knows can help us out here go ahead).
Glenn:
Excellent point, yes the tissue was healthy, that’s why I said “in this particular instance”. If the tissue was inflamed the Erbium might have performed poorly. However, I was IMPRESSED(get it?) that I was able to get this smooth of a margin with an Erbium laser. Believe it has to do with increasing the PPS to 30 Hz which gave me a nice smooth trough.
The camera is my same old Nikon Coolpix 880, I just took the pic at high resolution and cropped down to the prep so that it would appear well on this forum(roughly 600 pixels wide).
Al
P. S. No I did not use H202.
BenchwmerSpectatorI ordered the OpusDuoE at the ADA meeting last Oct, they were just showing this model. I got it in March.
It uses a hollow wave guide, it coud be a couple of inches longer, but it makes you keep it straight which gives you a truer power output. The cart has rollers and I move it inches either forward or backwards for upper arch vs. lower.
The handpiece is like a high speed in size, with removable sapphire tips, straight or tapered. I use 1000 or 800 micron for hard tissue, the small fibers 200, 400 are for soft tissue. I haven’t tried the 600 yet. They also have hollow 1300 metal tips for soft tissue.
Pulses can be set from 7-12 Hz. The foot pedal for firing can be set on variable, like your handpiece rheostat, you can decrease the Hz from your setting, by letting off the foot pedal.
I liked the ability to vary the number of pulses and tip sizes.
I’ve been using an Nd:YAG since 1999. I’m still learning uses and technique on the Erbium.
Jeff
Lee AllenSpectatorGlenn,
Interesting as usual. I have a similar case that is bite sensitive without thermal and found a distal marginal crack (one) similar to what you are showing, but after using a waterlase at 3.5W to remove enamel around the crack and some of the adjacent composite and placing a flowable, it has not resolved. You implied that this one did. Did it take time or was it noticed immediately?
Mine is 4 days Post op and still noticable. I am contemplating removing all of the composite to check for a more extensive crack but feel that I may want to give it some time to resolve the pulpitis.
Any thoughts?
2thlaserSpectatorLee,
What I have found in MOST of these cases is you HAVE to remove all the composite, laser the crack as far as you can see it, then place a new restoration, making REAL SURE the occlusion is adjusted correctly. I have had very good success with this. Glenn, what is your take on this?
Mark
2thlaserSpectatorHey Bob,
I can teach you how to do crown preps!!! uh…..ok, well, being Italian….Welcome to the Family!
Mark 😉
Andrew SatlinSpectatorHi Jeff,
Looks good. I see a fair amount of cases like this and I feel that they are among the most difficult to treat with conventional resective surgery. You made it look easy.
I was curious if you used the standard 360um fiber for this case.
Andy
Robert GreggParticipantHi Al,
Nice going!
Yeah, as far as pulse duration for the DELight goes, Tom Haney told me it will vary in the software matrix as you change the Hz. So it is not user controlable, but will vary from 210 to 240 as you increase your repetition rate from 15 to 20 to 30.
Tom?……..oh Tom???
Bob
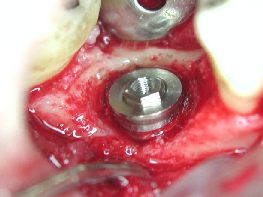
Kenneth LukSpectatorPatient returned for stage 2 implant treatment symptom free. A pin hole sized pus was draining on the ridge.
CONTAMINATION!
Flap was opened and granulation tissue was all around the implant. The implant has already osseo-integrated.
All infected tissue removed with 980 under saline irrigation. At the deepest bone level, the implant surface was lasered circumferentially.
Area infected limited to under 2 polished threads of 3i implant, no bone augmentation done. Flap closed with healing abutment.
After 4 weeks, impression taken and crown cemented.
Ken(Edited by Kenneth Luk at 11:03 pm on June 4, 2003)
SwpmnSpectatorThanks Bob. You and I had this conversation previously on PD and I thought it was around 240 usec. I’ve looked through the manuals for a PD spreadsheet at different settings like you mentioned in a post to Glenn. Haven’t found so far, hopefully Tom can help.
Al
Kenneth LukSpectator



Hope the photo sizes are ok
Ken(Edited by Kenneth Luk at 2:00 pm on June 5, 2003)
ASISpectatorHi Jeff,
Looks good.
What’s the deal with biological width? I’ve noticed it being mentioned in a couple of your posts. An inside joke?
Andrew
-
AuthorPosts