
Forum Replies Created
-
AuthorPosts
-
ASISpectatorHi Allen & Glenn,
I concur with your assessment, Allen.
It’s not called Viewmax for nothing.
I did some hard tissue treatment today. Really enjoying it so far. The patients are pretty as well.
Andrew
ASISpectatorThe patients are pretty happy that is. Although some of them are pretty as well.
Andrew
ASISpectatorHi Glenn,
Please keep us updated on your Delight.
Andrew
Glenn van AsSpectatorLee ……thanks.
I try different things……am willing to put my neck out and am fortunate to be able to take photos through the scope easily ……..
The flowable for small lesions works nicely. I like Point 4 flowable for the Class Vs and it is very plasticky…….works nicely.
I hope that with time we can all get a chance to meet……..
I enjoy this forum for what I learn…..I have to redo the endo on the 2nd molar and will try to get a temp crown or an ortho band on the tooth………
Thanks for the advice………
Cya
Glenn
Glenn van AsSpectatorVery nice pictures Jeff…….nice service for your patient.
I am always concerned with caries still left behind.
With all the erbium lasers I hate using Caries Detector Dye and in addition there is no tactile feel for when all the caries is gone. How do you determine if all the caries in a case like this where it may appear in the prep photo like decay is still there has been removed. Do you use round burs, CDD, spoons….
Do you use GIC in the base……its something I find tough to treat with the ErYag on soft caries cases and that sometimes the caries still is present…….
Glenn
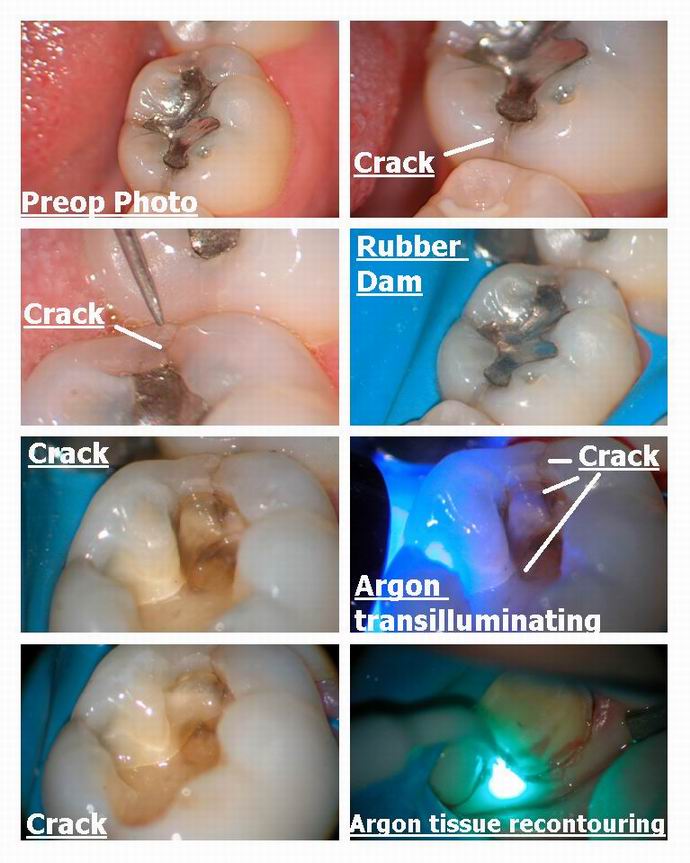
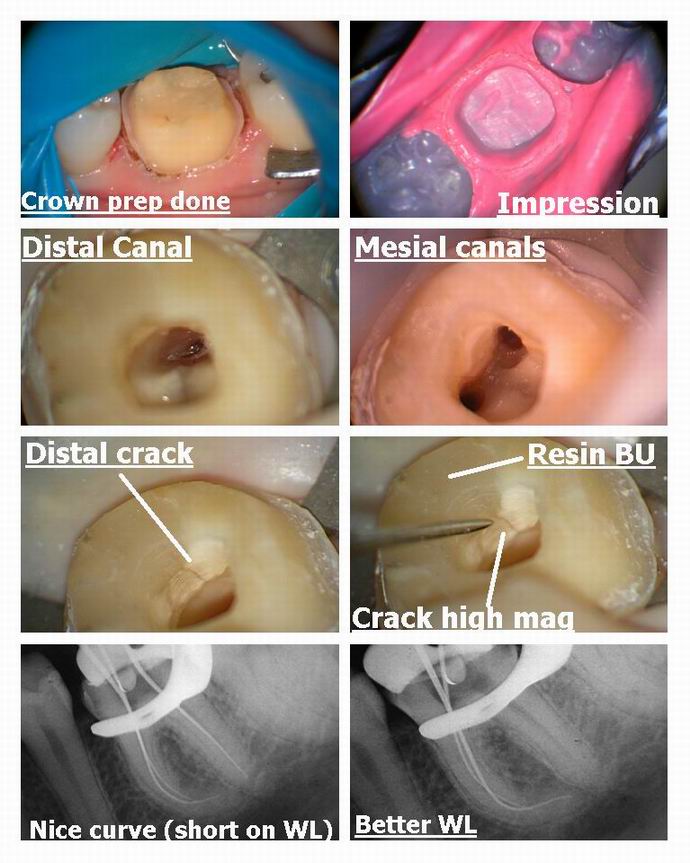
Glenn van AsSpectatorDo the endo……..here is one of my dental assistants teeth, lower left 1st molar that was sensitive to chewing, never settled down………
She had the composite done…..no better.
Gold crown done……temp cemented no better…….pain to chewing.
Did the endo yesterday……….
Note the crack……..my dental assistant Lori saw it when I was working and she saw it on her monitor and told me…and I told her thanks….I never noticed it when we were doing the open and drain……..nice curves huh.
THats why I LOVE THE SCOPE.
glenn
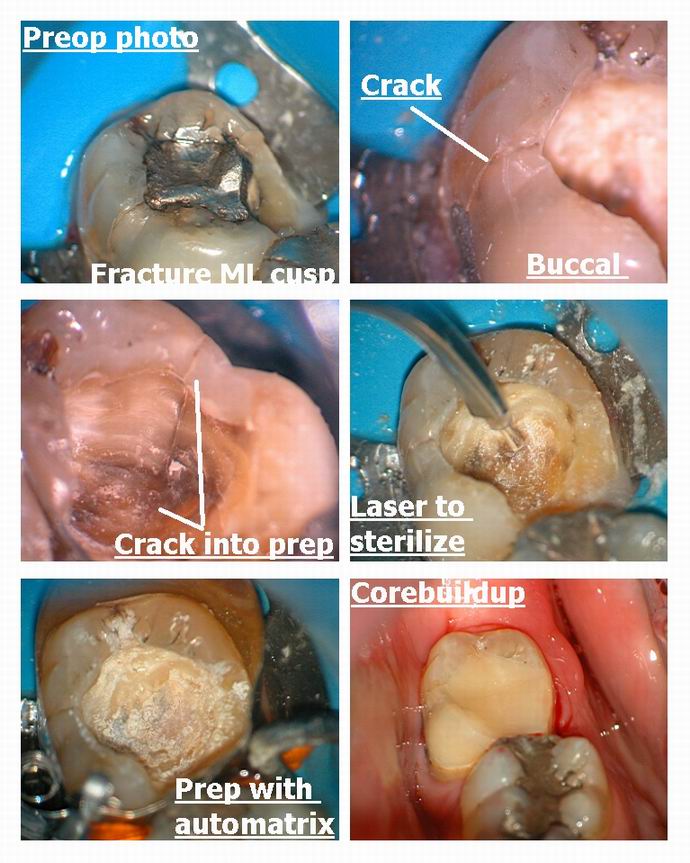
Glenn van AsSpectatorHere is another one from yesterday slated for a crown.
Patient broke ML cusp of on old amalgam.
Showed patient crack on buccal which was asymptomatic.
Once amalgam removed (with anesthetic) then noted crack went right through to prep from buccal.
Advised patient on weakness of tooth and advised on crown…….showed him cracks…..( it was a cracked tooth kind of day)……..
Tooth not bothering him but he is booked for crown…..photos sold the crown prep which he obviously needs.
Glenn
Glenn van AsSpectatorHi Janet…….talked to Tom Haney today…….Don Coluzzi will do a section on the 810 diodent at LVI…….
So it will be included.
All the best.
Glenn
Janet CenturySpectatorTom got back to me too. See you there!
Regards,
Janet
Lee AllenSpectatorGlenn,
Wild endo. While I realize that not all cracks are created equal and some of the most innocent looking will involve the pulp, I infer from the answer that the lack of cold sensitivity cannot be construde as an indicator that the crack is a minor leak requiring only a conservative laser prep and fill.
My patient is returning today (day 5 post op) because it is annoying her. I was hoping for a definative answer other than endo, however that is still on the DD list. I will recheck the occlusion, test with the tooth sleuth and refill looking for a crack, perhaps one that was caused by composite shrinkage.
So, how long before your patient with the dual cracks and no thermal sensitivity recovered from sysmptoms?
Inquiring minds want to know.

Glenn van AsSpectatorYou Know Lee this is an interesting question……..
I havent heard back from the fellow with the dual cracks but they werent very deep at all.
I find cracks that run Mesial to distal ( the endo tooth) are bad ones and often involve endo……
In general if the patient has significant cold and hot sensitivity AND Chewing sensitivity I tell them that they are probably looking at endo + crown.
IF they have just chewing sesitivity then I tell them they MAY need endo but there is a good chance that only a crown ( or a restoration if the crack is small) will be needed.
One good thing with the scope is the ability to document these cases……..its wonderful to show the patient the crack..helps medicolegally.
I have found that some patients live with the chewing discomfort and chew on the other side while others just cant handle it.
I have tons and tons of these cases documented and Dr. David Clark has written an article for the Journal of Esthetic and Restorative Dentistry magazine that attempted to classify these cracks BEFORE they become endstage and symptomatic…….
The scope is awesome for endo , decay detection, cracks, placement of margins , crown inserts, laser dentistry (seeing how far the tip is away from the tooth, troughing on crowns effectively) just to name a few things off the top of my head.
Cracks are tough to treat at the best of times but I would strongly suggest adjust the occlusion once, remove the restoration put a temp in if you wish but patients want results and they want the pain to go away. Being able to show them the cracks and head in the right direction …….(crown +/- endo) is at least heaing them there.
Let us know how your case ends up……..hopefully it is a simple solution but unfortunately it isnt always.
One last thing……its amazing to see how many teeth crack after the bur enters into the occlusal pits…..not always polymerization shrinkage………I have seen this with my own eyes with crosscut fissure burs on occlusals.
Like a lightning storm……………
Good luck with your patient……
Glenn
ASISpectatorThanks, Glenn.
The voice of experience is heard loud and clear. For your scoped eyes have seen much that many unaided eyes or lesser aided eyes have not been able to.
Thanks again.
Andrew
BenchwmerSpectatorAndy, Andrew,
All my Nd:YAG cases are now done using the 360micron contact fiber from MDT, Before this year I used 320 micron fibers. These new fibers seem more durable.
The reference to biologic width come from my Dental Town Case presentations and a case published in the DTown magazine in February, one anti-laser heckler could not get off me on biologic width. Glenn and others now include pictures w/ a perio probe on laser cases to keep the subject from starting again.
dilbertSpectatorstatus report as of 09/18/03 (no changes from 06/24/03)
number of failure reports: 4
number of no-failure reports: 1
number of models: 3
number of hard tissue lasers:2
number of soft tissue lasers: 2It will take much more data to generate meaningful charts. I will periodically edit this post to keep interested people up to date.
So far all owners of failed hard tissue lasers feel that their failures are a direct result of very inadequate training(aka self training).
If the manufacturers are monitoring this thread: DOCS NEED ACCESS TO IMMEDIATE TRAINING AT OR BEFORE DELIVERY.
(Edited by dilbert at 8:10 pm on Sep. 18, 2003)
BenchwmerSpectatorGlenn,
I use Karl Schumacher spoon excavators (#045) or a small round burr to remove the final debris and insure hard surface to bond to. These spoon excavators are so small, on a penny the excavator head only covers one number on the date. I’ll post a photo later.
I use no bases or liners (not since 1995), just a dentin bonding agent, in this case I-Bond.
Jeff -
AuthorPosts