
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorNeat result Jeff…….looking back I think a tad of osseous would have helped here just prevent the slight rebound.
You could do it now but I am sure the patient is pleased.
There was 1mm to 1.5mm rebound though. This is tough to get perfect….
You did a beautiful job.
Clap clap clap
Glenn
pfgettySpectatorA lot of you guys have long ago posted and talked about the basic stuff………..pedo preps, class two preps on molars and premolars, etc, etc,
But I don’t have a laser, and if you are doing this stuff I’d love to see cases that aren’t 4 years old…………I know you guys are doing these still and to you they seem routine, of course. But you know more than you did a few years ago when you started doing them. So how about some updates and show how the preps should be prepared, how you remove the decay, how you finish the margins, the use of acid etch and bonding, whether you could use Fugi IX if you wanted, etc. etc.?
toothsloothSpectatorGlenn,
I have some that I got from N.O…I’d be happy to share some with you if you need it soon. Just give me a ring and I’ll send it over!
Regards,
Jimmy
dkimmelSpectatorA challange??
A call to action??
You are correct in things are not the same as 4 years ago…This is a tough time of year though to ask. One very busy last day of the year for me tomorrow…
I’ll have to get back to you in Jan….
David
pfgettySpectatorThanks for the reply, and I am in no hurry at all.
DrDanSpectatorI shouldn’t have posted that last post. I think I “jinxed” myself. We finally had ONE person this week we had to drag out the syringe for……so we could do it the “old fashioned way”.
Seriously…..going 2 months between failures isn’t so bad!
Dan

jetsfanSpectatorI am in need of some assistance with this diagnosis and since I know there are so many quality people on LDF I figured I’d ask you guys and gals.
This 10 year old girl presented to me today with these two reddish desquamative areas in her mucosa above #8 and #10. She is in perfect health and has no habits like placing objects in her mouth. They are slightly tender and the mother is concerned. I saw her last year and she had similar lesions above 8 , 9 and 10. I treated them as I would an aphthous ulcer at the time. (.25W 11A)The mother says they really have not changed (except that #9 is no longer present). Anyone have any thoughts on this?
Thanks
Robert(boy is it tough to be a JETSFAN)
https://www.laserdentistryforum.com/attachments/upload/10 yr old girl.jpg” border=”0″>
jetsfanSpectator
here’s the photo.
Glenn van AsSpectatorHey Jimmy…..some what?
Glenn
PS I have a cool case of Osseous that I did recently like this I might post in a day or two.
Cya
Glenn
Glenn van AsSpectatorPaul……..you are on. I will begin to post the small stuff. The stuff everyone buys a laser for and then moves on. I will start by saying that for the most part I use the laser for restorative dentistry in the following situation.
1. Pedo (kids are great with the laser) especially the interproximal back to back lesions on the primary molars.
Great to do without anesthetic but you have to develop soft touch on the tissue with matrices and topicals work great for that.2. Adults
Class 1 and 2s that are small (ie less than 40 on the diagnodent) and only Class 2s where the patient is adamant that they want it done with the laser. ITs slower and I charge more for it.
Anterior Class 3, 4 and all Class Vs are great with it. Its not a panacea for all but I tell you , patients love it when it works.
You need to use resins or GI for these preps as they are rougher, so amalgam is not possible.
I will post some “beginner ” stuff or bread and butter stuff over the Xmas season as time permits.
Hope this helps you but many buy the laser in the hope of being faster, being able to do tons without anesthetic but as my good friends Kimmel, Williams and McNamara say, the key is to success without anesthetic is patient selection and trial and error gives you some idea as to what will work without anesthetic and what wont.
One change in settings that has occurred over the years has been a gradual reduction for enamel ablation from Higher Hz rates (pulses per second ) to lower Hz. In the old days most of us would use 30Hz on the Delight and on the old Waterlase it was always 20Hz as that was the only setting. Alot of Opus users were able to penetrate enamel at 10Hz and very high energy per pulse (the Opus Principle or the Jackhammer (high hertz) vs the Sledge Hammer (low hz) effect).
Effectively this did a couple of things. It gave more time between pulses for tissue relaxation and each pulse was at a huge energy compared to the old days. More chance of success in decreasing sensitivity during the preps.
In addition another change I have seen is in the bevels on Class Vs, 2s etc at the cavosurface margins.
More and more people are using lower energy settings and higher Hz for a smoother cut that doesnt give such a big ablation crater per pulse. What these big ablation craters did was decrease bond strength leading to staining at the enamel margins so people now use say 40-50 Hz and 30-40mj which gives a smoother margin and better bonding. I will scrape the margins with a spoon, some use a diamond , others AA.
One last suggestion for someone looking into lasers. Make sure that you are using good magnification for laser dentistry. Loupes above 4.5X make it far easier for the hard tissue lasers and to a lesser degree soft tissue lasers to see what you are doing. Hard tissue lasers depend far less on tactile ability than do other aspects of dentistry. You dont feel what you are doing , but you must see what you are doing.
Hope that starts you off on the right path.
Glenn
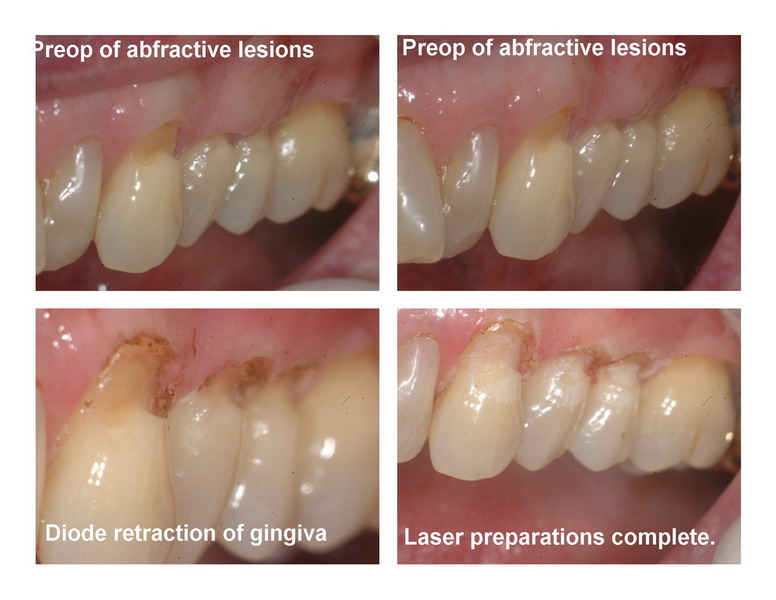
Here is one case where I did some Class Vs
Diode used at 0.8w pulsed with TAC topical.
Erbium for preps on Abfractive lesions (patient wouldnt go for grafts and it was sensitive). 50 Hz and 30-40 mj on enamel for bevel.
Point 4 opaque flowable for material.Simple, no anesthetic laser preps.
Glenn

(Edited by Glenn van As at 2:36 pm on Dec. 22, 2005)
(Edited by Glenn van As at 2:38 pm on Dec. 22, 2005)
Glenn van AsSpectatorOne more before I go back to work. Here is one recently on a canine without anesthetic on the lower. A class 3. I nicked the adjacent tooth with the laser for 3 pulses as you can see. THe initial entry on this was at 10Hz and 220 mj into the enamel. Decay removal at 20Hz and 100 mj and finally bevel at 40Hz and 50mj ( a little heavy for me).
I placed the restoration in with a hybrid , Gradia.
Gotta run, hope this helps. Off to do 2 occlusals with the laser. Will post them.
Glenn

Andrew SatlinSpectatorHi Glenn!!
When you say osseous now you do mean open… right?
With sutures and sensitive roots and black triangles?
Why not just extract and place implants?
That seems to be the reputation most of us periodontists have been accused of lately.
Pardon the sarcasm, I have just been reading alot of anti – periodontist posting recently on this forum and I find it a bit alienating for those of us who enjoy being here.
Truth is I would love to see your cases when you get a chance to post them.
andy
Glenn van AsSpectatorHi Andy……did I say with sutures, sensitive roots and black triangles recently?
If I did then I apologize.
I do believe that the current push in perio is more a concentration on implants and Connective tissue grafts , more predictable than periodontal therapy and less sensitive than full flapped osseous.
I also know that you have a penchant for trying to save teeth, hence your interest and usage of the NdYAG.
Not all marbles are the same size or color.
Finally, I have cases of closed and open flap that I have been doing. I am getting some interesting results. Some of the closed look great, some look ok. Some of my open look worse than some of my closed. Want to know why.
I dont handle the tissue as well as you , hack2 or Danny. That is your area of expertise and you guys are masters at that.
In any event , there is alot of room out there for lasers. Lots of cool things that we are always pushing the envelope. I for one am not so bold to put these up now because people seem to get all upset and anxious about whatever I am trying to do.
Some say that people will copy it, others say its not right to teach this….
So its easier to post the simple stuff here, but suffice it to say that I am getting feedback on stuff, because I am trying to figure out how the laser fits into the osseous world.
Some would say it doesnt, I wouldnt. Many of my patients might not either !
Andy, all the best and keep trying to save teeth, have an open mind to lasers (I know you do) and you will always be in my mind a winner!
Cya and happy holidays.
Glenn
Andrew SatlinSpectatorHey Glenn,
I am sorry if it sounded like I was accusing you in any way. That was not my intention. In fact I applaud you for educating yourself in both open and closed surgical procedures. As you know I feel both are appropriate on a case by case basis.
I suppose CT grafts and implants are somewhat more rewarding than the conventional osseous surgery but I believe perio treatment is still very much focused on regeneration. Hence, my personal interest in the periolase.
Anyway, Best regards to you and your family for the Holidays.
Sincerely,
Andy
Glenn van AsSpectatorHi Andy……I have come a long ways from my first stuff. To be honest, David Kimmel and others like Matt Brink have a far better understanding of the elements of periodontal surgery than I do. I am weak still in osseous and its details. I know that in some cases for me closed flap is easier to do than open flap because as mentioned I am not as good in handling the flap and tissue as Danny or others.
I know I will never get as good as Danny as even with my scope and being able to see details, he is a surgery god.
I appreciate the patience that some here have shown me. I must admit that I at present am not to excited to show closed flap cases despite the fact that I am doing them for various reasons. I am trying to gather 100 different cases and also get followup on osseous done with the laser. When I get cases that are 2-3 years old , (they are starting to come) then I feel more comfortable.
Oh I will post the final photos of the vertical root amp that Danny showed me how to do. It worked out AWESOME.
The crown is not perfect in contour but the tooth looks great…….
Look for that one…..I am off to find the photos and put them in a collage.
cya and thanks for the nice words, I tell you though, this osseous is a whole other thing.
PS Danny sent me another case, I am off to look at that now, I do learn lots of things, so many details to study and understand about biology and then also to see where things fit in.
I might send him a case of anterior closed flap I did recently in private if he promises to look at it and see what he thinks with an open mind…..it was done because the girl who was 17 wouldnt have ortho, and wouldnt have a surgical flap. I talked to her for a huge amount of time and she finally succumbed to the laser but not to the open flap.
In any event there were some interesting results so far after only 1 month mind you.
Gotta run……
Glenn
-
AuthorPosts