
Forum Replies Created
-
AuthorPosts
-
etienneSpectatorHi Guys
I just saw this patient again when I completed the endo. This is the clinical picture:
Here are the pics taken on 26May and today, 12June.
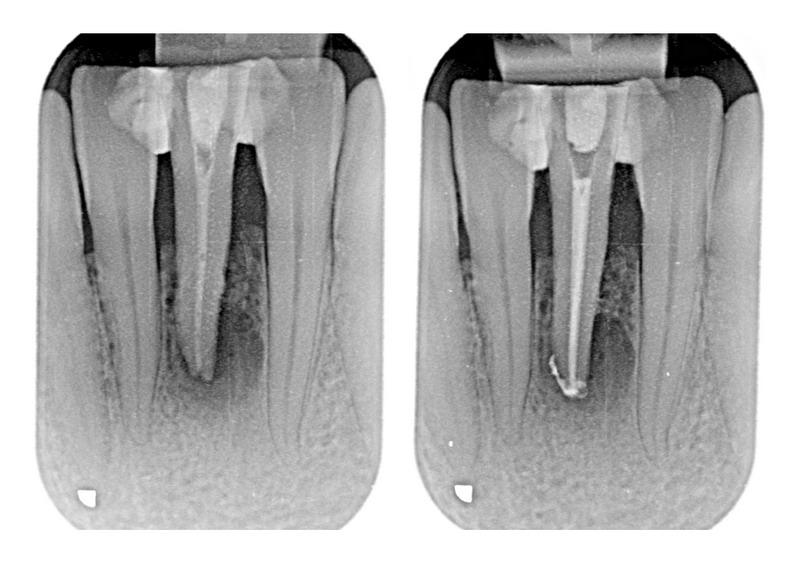
It would be interesting seeing her again in a month or two.
Any thoughts?
Take care
Etienne
JerryDSpectatorHerb,
Interesting stuff. A patient of mine has a LLL. He is not a doctor, but he treats “patients” with this laser, and talks about some pretty hard-to-believe ideas, including curing Lou Gehrig’s Disease (potentially).
My question is, how do you think DDS responds to the use of a well-made Tanner appliance?
Jeff
BenchwmerSpectatorBob,
Some of the time I do it as a favor to the Endodontist and patient.
When billing I use the code D07510 Incision and Drainage Intraoral (My fee 趁)
Jeff
Robert Gregg DDSSpectatorNice endo. Time will tell………
Take care,
Bob
czeqm8SpectatorThe ADA has come out with recommendations. Of interest is the following:
They do not recommend prophylactic antibiotics routinely.
In addition, immediately prior to and following surgical procedures involving bone, the patient should gently rinse with a chlorhexidine containing rinse. Typically, chlorhexidine is used two times per day for two months post surgery. This can be extended based on how the patient is healing.
Prophylactic antibiotics may be utilized during the healing/wound closure phase, for procedures that involve extensive manipulation of the bone (e.g. extractions, periodontal recontouring, sinus lifts etc.) but is not mandatory nor even recommended. Use of prophylactic antibiotics depends on the clinician’s level of concern relative to the individual patient and their specific situation including concomitant risk factors (i.e. prolonged use of oral bisphosphonates, older age, concomitant use of estrogen or glucocorticoids ∗). In some situations, prophylactic antibiotics may be instituted a day or two prior to the procedure.
I think that we should be just fine with our normal LANAP routine, but you might want to increase the chlorhexidine just to be safe.
Go to the ADA website for a complete list of recommendations.
(Edited by czeqm8 at 7:06 pm on June 15, 2006)
SwpmnSpectatorToday I attended a Laser Dentistry overview presentation given by a highly respected clinician with long term involvement in laser dentistry. Presentation was very positive with regard to applications and mentioned all of the major manufacturers. Here’s what bothered me:
1) Implication that Er,Cr:YSGG wavelength is superior to Er:YAG wavelength:
2) Er,Cr:YSGG wavelength cuts one third faster than Er:YAG wavelength
3)Er,Cr:YSGG wavelength facilitates hemostasis better than Er:YAG
4)Er,Cr:YSGG is much more efficient for ablation of soft tissue than Er:YAG
5)Er,Cr:YSGG wavelength ablates via a phenomenon termed as “Hydrophotonics”. The water spray with the Er,Cr:YSGG laser actually does some of the ablation. The Er:YAG laser only uses water spray as an irrigant, and to quote the speaker “Cuts like a hot poker”.
Although the presentation was very positive, I felt bad as I looked around and saw the unknowing audience nodding their heads.
But……………it wasn’t my party.
Al
etienneSpectatorThanks Bob! Yep, wish it would hurry up though…;)
Take care
Etienne
Robert Gregg DDSSpectatorEtienne,
Such a typical dentist!
Instant gratification you want? LOL! We were all trained that way. Unlike physicians.
Great things take time to realize. Like waiting for the sun to come up, then it’s always darkest right before dawn.
Take care my friend,
Bob
dkimmelSpectatorAllen are you over in Orlando this weekend???
If so watch out for Katie she is running aound over there this weekend at the meeting…
AnonymousSpectatorAllen, can I be the 1st to guess who sponsored the speaker? :biggrin:
jetsfanSpectator


Here is an interesting case I saw Friday afternoon. !5 yr old boy with a history of petet mal seizures since birth. Taking Dilantin 100mg tid, Phenobarb. 10 mg tid (I believe). His DDS did an exam and prophy and sent him to oral surgeon for gingevectomy. Oral surgeon took one look and said he should be seen by a laser dentist so he was referred to me. He was premedicated as a precaution by his neurosurgeon.
YOu can see his preop anterior and max, occlusal view.
Obviously this child needs quite a bit of treatment. As he was going to a school dance that evening I decided to treat the max. anterior in the limited time available to us. I used Ron ‘s DRK topical for approx 5 min. I proceeded with the Waterlase using a g6 tip at 5W 11%A. to carve away the tissue immediately around the centrals careful not to affect the enamel( which did happen in spots). As this was going very slowly and there was so much to do I upped the wattage first to 1W and eventually 1.75 w 13%A 10%w using Mark’s C3 tip to essentially festoon the fibrotic gingiva much like you would a denture wax up. He felt nothing , essentially no bleeding, no post op pain. He had a good time at the dance. He and his parents were extremely grateful.
Comments and suggestions about this and future treatment for this patient would be appreciated.Robert
etienneSpectatorHi Bob
How are you doing?If I used twice the power, would I have half the healing time??? 😉
Just kidding of course.
I was accused today (only half jokingly) of changing the dates on the pictures of these cases. The parameters of what can be done seem to be changing all the time.
Take care
Etienne
SwpmnSpectatorExcellent service Robert! I can see why the patient and parents were grateful.
Kaminer’s DRK Liquid works really well and is now the only topical anesthetic we use. Many times I add a drop of methylene blue just so I can visualize exactly where the topical has been applied.
Al
jetsfanSpectatorDoing some research on lasers and epilepsy and found and article stating that non invasive laser therapy is contraindicated in epileptics(see article below). I did not realize this. Is there something that refutes this? Do I not continue with laser gingevectomies for this child?
Contraindications in Noninvasive Laser Therapy: Truth and Fiction
Author(s): Leos Navratil MD, PhD ; Jaroslava Kymplova MD, PhD
Source: Journal of Clinical Laser Medicine & Surgery Volume: 20 Number: 6 Page: 341 — 343
DOI: 10.1089/104454702320901134Abstract: Objective: Noninvasive laser therapy is a treatment method employed in many disciplines. This review article points out instances when it appears to be effective to administer such therapy. Materials and Methods: Noninvasive laser therapy has a number of suitable applications that cause minimal damage to the patient. Many patients are not sent to institutions equipped with relevant instruments, since physicians are burdened by a number of contraindications, many of which are incorrect. The purpose of this article was to divide these contraindications into the following three groups: correct indications, indications doubtful under certain conditions, and incorrect indications. Discussion: We consider the following contraindications as correct: history of a histologically demonstrated malignant carcinoma; irradiation of the neck region in hyperthyreosis; epilepsy; exposure of the retina; and exposure of the abdomen during pregnancy. The contraindications that are doubtful under certain conditions are as follows: fever and infectious diseases; certain blood diseases; heavy blood losses; neuropathies; and irradiation in the region of gonads. The other contraindications reported in the literature are considered to be in
Robert Gregg DDSSpectatorHi Etienne,
I’m doing fine, thanks. And you?
If I used twice the power, would I have half the healing time???
In this case, you could have probably gone from 35 Joules to 70 joules w/o any problems, but w/o any better healing time or benefit either. “Less is more” in these cases is the way to lase.
Take care,
Bob
-
AuthorPosts