
Forum Replies Created
-
AuthorPosts
-
Andrew SatlinSpectatorRobert,
I have never heard of the contraindications as stated by that article either. I am going to ask around about that.
I have treated several of these cases over the years. They are difficult. They often rebound and can be very dose dependant. You can consult the physician but rarely will they chage meds because of medication associated gingival overgrowth.
My best suggestion is to stress oral hygiene with these patients. Better plaque control is the most effective way to reduce the hyperplasia. On a fifteen year old patient you have really got your work cut out for you.
Anyway, the treatment looks very well done. Keep us posted.
Andy
SwpmnSpectator
jetsfanSpectatorAfter doing more research and speaking with Paul Bradley, and Mark Colonna I am convinced there is no contraindication to treating epilepsy patients with ER CR YSGG wavelength. Perhaps a case may be made for lasers in the visible spectrum being contraindicated.
Robert
dkimmelSpectatorAllen , Can we get you to present this case at the next TBLG meeting?
SwpmnSpectatorQUOTEAllen , Can we get you to present this case at the next TBLG meeting?Sure. We “wooof” planed my golden retriever that day as well! Later on I may need to bring them to Hudson(oops, Bayonet Point) for LANAP, LOL!!!!!!!
I took the pics to their vet. He was fascinated since he always uses sedation. Asked to keep the pics for a planned collage. He told me canines mostly have problems with calculus deposition on facial surfaces, that the tongue does a fairly good job removing plaque on lingual surfaces.
Apparently some veterinarians use lasers for certain types of surgery.
SwpmnSpectatorDid a surgical extraction of a lower molar using the chisel tip with my DELight. After we got done, my assistant said “What the heck was that?”. Ablates tooth and osseous like a hot knife in butter.
Have been doing some work etching occlusals of molars with 35% phosphoric acid prior to erbium ablation. It does seem to initially increase the speed of ablation. But once you get through the shallow layer that is etched, seems to slow down. Almost like you would need to stop and re-etch.
This morning I was so glad I had my erbium. Developmentally challenged child came out of hygiene with occlusal caries on #31. Child was very nervous, fidgety and had limited opening. I was able to sneak my 80 degree tip in and prepare the tooth without chemical anesthesia.
dkimmelSpectatorAllen
I know what you mean.. It is real quite…..I quess its just summer.
The only thing we have been doing is using the chisel tip for bikni hair removal.. It works great. Still find I need the loops……
JanetCenturySpectatorThank you gentlemen for all this info and wealth of experience. I upgraded a month ago, but I’m just finally sitting here on a day off and playing with the different new settings and this thread was a world of help.
Thanks!
Janet
2thlaserSpectatorHere you go Allen, first ever complete laser root canal on a canine…

60mm MZ-2 fiber

Obturation with EndoRez from Ultradent
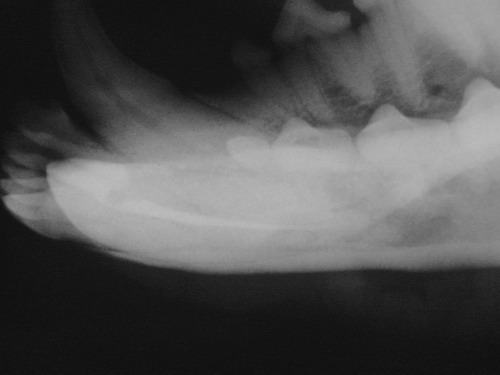
Final Radiograph….
Whaddya think???
Mark
SwpmnSpectatorGeez!!!!!!!
Nice work. 60mm?
 ??
??That’s cool, Mark!
Al
SwpmnSpectatorQUOTEThe only thing we have been doing is using the chisel tip for bikini hair removal.. It works great. Still find I need the loops……Well with your staff I’m sure that keeps you very busy during the summer months:shocked: .
dkimmelSpectatorSince poor Allen is bored I got an idea to spark some life back into this thread.
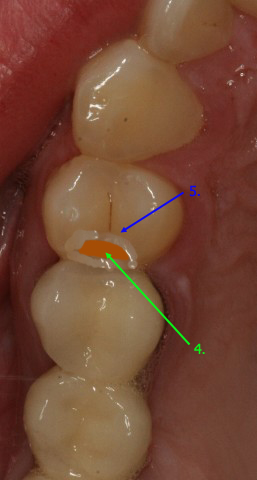
Lets compare settings. Below is Tooth #5. It is a virgin tooth on a 25 Y/O male. There is decay on the DO. It is moderate in depth and an RCT is not indicated. Non phobic.1. What laser would you use?
2. Will you numb the patient?
3. Will you do the 90sec. pre laser anesthic?
4. Intial settings . Tell us in focous or not in focus and how you would change your settings as you progress.
5. Tell us what setting changes you would make if the patient started to get sensitivity.
6. At what point wouuld you numb the patient?
7. Tell us also if you would use a handpiecie at any point other then to polish the filling. Also if you use any hand instrutments??This should be interesting.

dkimmelSpectatorOk, I’ll start.
If I used the MD: loops x6I would not numb the patient nor do the 90 sec prelaser stuff. Instead I would use a G6 tip at 10HZ 23%water, 60% air at 2.00 Watts. Staying in focus I would start at a right angle to the marginal ridge and alblate away. If I felt I was not cutting fast enough I would bump up to 3Watt a little at a time. Too fast or getting sensitivity go defocused. Of course as I go into dentin I would just defocuse. Remembering to keep the tolet bowel prep form to keep pooling water. As I go into dentin ,if sensitvity was a problem I would change to a Z6 tip.
Once into caires if I feel the laser is stalling I will go to MArks Spoons. I don’t use a bur. I will sometimes use caresol if it is a large lesion, pretty rare to do this.
Caries gone, I use the Z-6 tip at 50HZ, 23%water,60%air at 0.5watts and start to bevel the edges of the prep. Then lastly spoon the surface to remove the molten enamel.
If I use the WAterlase: Still loops x6
Still I will not numb but will do the 90sec laser treatment. G4 tip, 6W 30%water 40% air.
Again starting at the marginal ridge. Dropping down to 2Watts averaging 3watts in focus. Changing as needed by seeing what is happening. With sensitivity I will defocus, change to a Z6 tip, drop the watts and drop the water % last. Once in dentin/caries just defocus.
Same as the MD with spoons etc. Finish the margins with just a spoon.The Delight: loops x6
Oops to follow. Susan is calling.
dkimmelSpectatorThe Delight
Loops X6
10HZ 120mj 30 deg tip focused Then pretty much the same as with the MD .
In the dentin defocus , pretty much like with the MD.
To finish I’ll go 30Hz 50mj in contact to bevel the margins.
If I get sensitivity I will defocous, Still a probly I’ll drop to 3 HZ..
AnonymousSpectator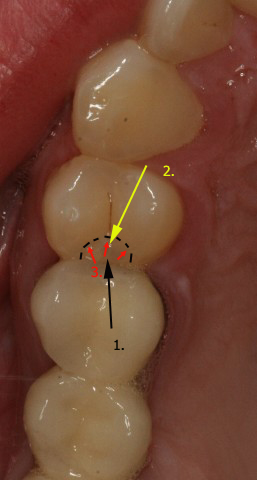
Versawave
10/400 defocused. 10Hz.Scope 8x1.Aim 1st from the distal toward the marginal ridge
2. then move and angle from the mesial toward the marginal ridge (best to place matrix).Remove enamel. Aim next vertically.
3.Next come from distal, again aiming at the side of the enamel rods of the occlusal table to widen out margin of prep and allow access.Stay out of dentin at this setting.
4. 10/180/10Hz. defocused to ablate or soften/hydrate caries. Focus 10/100/10Hz for caries removal then Colonna’s microspoon or round bur. Repeat until sure caries gone.
5. 10/100/10Hz (usually don’t change Hz unless soft tissue or doing laser analgesia) very defocused or slow speed round bur run over edge to create small bevel and remove inorganic byproducts.
Patient would be numbed if they preferred or I wanted to ‘move things along’ a little quicker. Also depends on if they’ve had previous laser experience.
No laser pre-analgesia.Haven’t used my Waterlase in 6 months but NLT will repair in 9 more days. If doing with Waterlase-8x scope.
4 watts 20 Hz 90 sec.50% air water differential for laser analgesia on occlusal. Prep the same except 4 watts defocused for enamel removal the 2 watts defocused for dentin. 1.5 defocused for caries (as best as I can recall 😉 ) -
AuthorPosts