
Forum Replies Created
-
AuthorPosts
-
whitertthSpectatorlooked like decay to me to but i couldnt pick anything with a sharp spoon, didnt fee like it with a round bur and she was starting to get sensitive so ileft it…what do u guys do if in that sitation sensitvity starts..could even go in with one watt and minimal air and water?
Glenn van AsSpectatorHi Ron………dont get me wrong ……..I love your pics and your case.
Given the circumstances I would either go in one with a high speed quickly and say hold on or if you want go in with low laser settings, or leave it and put GI overtop but your case is great and your photos beautiful.
CLAP CLAP CLAP
glenn
AnonymousSpectatorOk, photo experts I need some quick lessons if you are willing. Got a Fuji to try out w/ macro lens and ring flash. Been playing w/ f stop and exposure .
1st taken 1/60 6.3

2nd 1/80 11

Both taken of my daughter at home in basement (yes I know its probably not the best place,but what can I say, I want to play with the camera:) )Suggestions/ Advice?

Thanks
drnewittSpectatorI use a coolpix 880 also, there are much higher pixels available now than when the 3.34 was tops but the 880 provides very nice shots. i still struggle abit with the focus. Feedback is welcome!. and shodows without the ring flash. the 880 has a nice close up feature but again makes it difficult to focus as the auto seems to not settle in and lock.
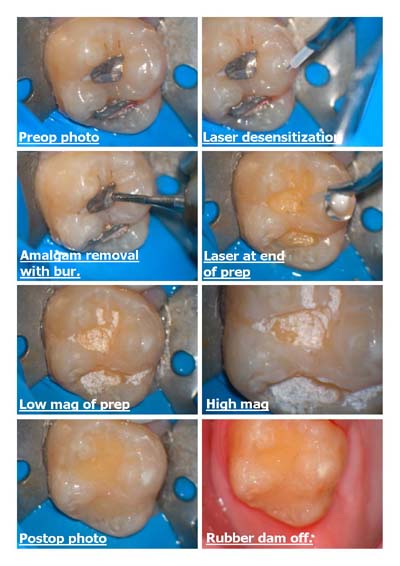
Glenn van AsSpectatorHi folks: A simple occlusal amalgam not that deep, but I had to try and do it without anesthetic. I used the laser for 90 seconds with a 400 micron tip at 4.8 watts and I let it run with water for that minute and a half all over.
Then I picked up a 557 fissure bur and used it to remove the amalgam and then used the laser to sterilize and disinfect the prep and get more retention.
All was done without anesthetic except for One touch topical from Patterson.
Patient was a 8 year old female , and pretty easy to work on but she felt nothing and as you can see in the 6th pic (after etch) the dentin was exposed in one area.
Just something for you to ponder.
Glenn
jetsfanSpectatorGlen,
I am unable to open any of your photos. Is there a special viewer that I need on my computer?
Jetsfan
PatricioSpectatorGlenn,
This approach is becoming my routine method of choice for small and medium amalgam removals especially on the bicuspids. I find it very successful and quick. I really appreciate your pictures they are a big help. Thanks,
Pat
Robert GreggParticipantGlenn,
What sort of change in post op sensitivity are you observing when you “Letch” (laser etch) the dentin??
I have noticed a considerable reduction, but there are times when I wonder if I need to also Letch the DEJ to be sure.
Thanks,
Bob
Glenn van AsSpectatorHi guys…of to bed gotta work in 6 hours. Had a hockey game and can never sleep afterwards.
Jetsfan, I dont think you need any viewer. What browser are you using ( I use internet explorer the most recent one) and it may be your settings on your browser.
Pat ……thanks for the kudos. Its really quite simple for me to shoot them and the magnification helps me alot to understand what is going on.
Bob……interesting you should ask. I posted a crown desensitization recently on here. The lady came in today and asked what I had done differently ( she has had quite a few crowns) and she told me that this time there wasnt much sensitivity and all the others there was. This was the one were I Letched (great great term) and then bonded overtop and Gary Griffin told me a while back that he was sure he was getting less sensitivity but I dont know if it is true or not.
Great question and I too often have to etch the dentin and then bond over it.
WHo knows………I dont think it can hurt.
Glenn
AnonymousSpectatorHi all,
Lady mid thirties presented today with this tooth(see xray below) 10mm pockets mobile. Went to periodontist last week who did probings and rescheduled next week for FMX and ext 4. Generalized 5-6mm pockets .No medical problems.
Lady desperately wants to avoid extraction. Any hope in scale and root planing followed by tx with diode (sorry Bob , couldn’t get her to go out to see you) and occlusal adjustment?
I’ve had pretty good success with 5-7mm pockets resolving but have not attempted any like this. I’m willing to try, she’s willing to try knowing she will still probably need ext. Is it a total waste of time? Thoughts? Suggestions?
Thanks[img]https://www.laserdentistryforum.com/attachments/upload/dmack.JPG[/img]
jetsfanSpectatorI know you guys and gals must be doing some perio with waterlase. I have dabbled in laser currettage, but am not really sure if I am doing it correct, ie is my treatment therapeutic or am I just going through the motions. I am looking for protocols that others have used successfully. Please include the tip used, settings, length of time per pocket laser is applied, when do you retreat, clincal appearance to know that you have done something efficacious.Oh yeah, anesthesia or not?
thanks for input.
JETSAN
AnonymousSpectatorjetsfan,
I considered using the Waterlase for currettage, as the people from Biolase were suggesting, but decided not to for the following reasons;
1. the tips only have end action- how do you do treat the inside lining of a pocket with something that is only has its effect at the tip with no side action?
2. the perio tips I saw were very inflexable-hard to get 360′ access to teeth
3.since the Waterlase seeks H20 molecules rather than pigment, how do you keep from affecting the hard tissue
cementum/bone?I think there are better choices – nd:YAD or Diode.
If you look up some of the stuff Bob Gregg has done with the nd:YAG or what Bob Barr has done with the Diode you’ll see some amazing results.I don’t think the same can be said for the Waterlase and perio tx. JMO
whitertthSpectatorwhat do u have to lose? I would try with no guarantees….if it works u have a nice case to publish…
Glenn van AsSpectatorHi folks : sorry for the long post with lots of photos but I thought it was a cool case with some nice photos.
Patient broke off the canine close to the gingiva , with some perio and I thought just after I started removing the composite overtop of the Gutta percha that I would document it.
I removed the gutta percha with gates Gliddens down to 16mm and then created a large post hole (6 on the fiber post (whaledent fiber I think it is) and cleaned the post space with the laser.
THe erbium yag laser with water removes the smear layer similar to edta and its visible with the scope as a much cleaner canal.
I then etched the surface to remove stain and get a more adherent surface for the bonding process. One tough part is staying on track when removing the gutta percha but the scope helps you so much in restoring these cases. Another problem is getting a dry canal without water pooling at the base and ultradents capillary tip suctions help there .
I got etch and bond down to the bottom and then cured with the laser which is small enough to fit down the canal assuring the bond to be cured. Then used a dual cure resin with the fiber post and cured around and on the post to set the resin.
BUildup done with composite and prepped quickly. Argon laser used to tissue retract and impressions taken to provide a crown for one of his remaining 4 teeth which is an abutment for his partial denture.
I thought all in all the pics were quite good and it was a fun case to do.
Hope you like it and I apologize for the size of the photos but I did edit them down as much as I could.
Glenn
You can find the pix on Sendpix as it was too big a case to post here on the forum.
Click on the link here
http://www.sendpix.com/albums/03012322/2238000000000858c0d7187a88dd9865c91be0596fc40d/
AnonymousSpectatorGreat case Glenn, thanks for posting it.
I can’t get over how smooth you are able to get the preps with that magnification. I’ve even noticed with the 4.5 loupes I’m able to make my preps smoother. I’m anticipating easier seating of restorations, have you found that to be true since working under the higher magnification? -
AuthorPosts