
Forum Replies Created
-
AuthorPosts
-
whitertthSpectatorpost was etched 360 degrees just not noticeable on picture….. sorry about the picture placement dont know what happened
Robert GreggParticipantGlenn,
Nice cases.
QUOTEi also am aiming for a diode to improve my soft tissue capabilities ( sorry Bob I know it should be an Nd:Yag but I am working it out in trade for lectures etc. with Continuum …..paying full price too.)No need to apologize to me……..I’m just sorry you don’t know the full range of capabilities of a pulsed Nd:YAG can do for your patients. Cuz you could do stuff that you can’t do now with your erbium or diode.
Hey, if you think I’d give you a discount, rest assured, I’d charge you FULL price too! And let you pay it off lecturing too…….MDT doesn’t compete with ConBio anyway. Neither the erbium and especially the diode aren’t in the same league as a pulsed Nd:YAG–especially the PerioLase MVP-7. It’s just the laws of physics.
Happy New Year!
Bob
whitertthSpectatorthe topic should actually be sculpture fibrecore post….sorry for the typo
Robert GreggParticipantWhat Glenn!!
Did you think I was invited?? I’m not going to Dana Point either, and it’s just a few minutes from my house!
Bob
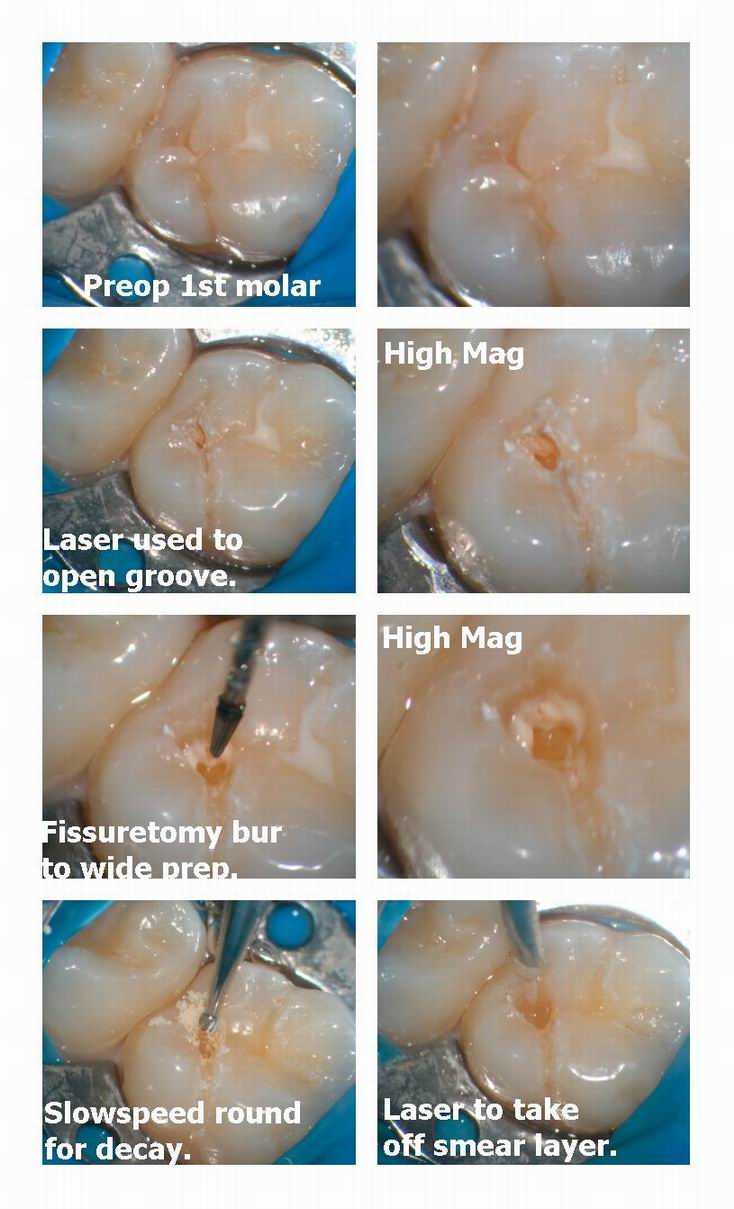
Glenn van AsSpectatorHi folks: in using the laser for small occlusals I find the major benefit is that even dental decay can be removed without anesthetic.
In my hybrid technique I am not adverse to using both the laser and burs.
Here is my technique from now on called the Hybrid Occlusal Preparation ( HOP) for short because I am hopping back and forth between the laser and bur to achieve the preparation without anesthetic.
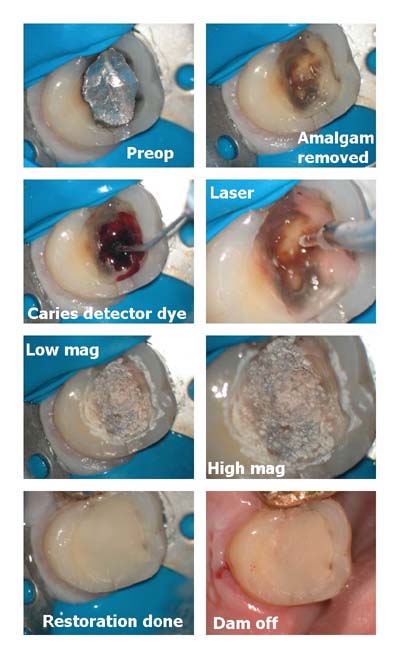
Here is a case I did yesterday using the HOP technique.
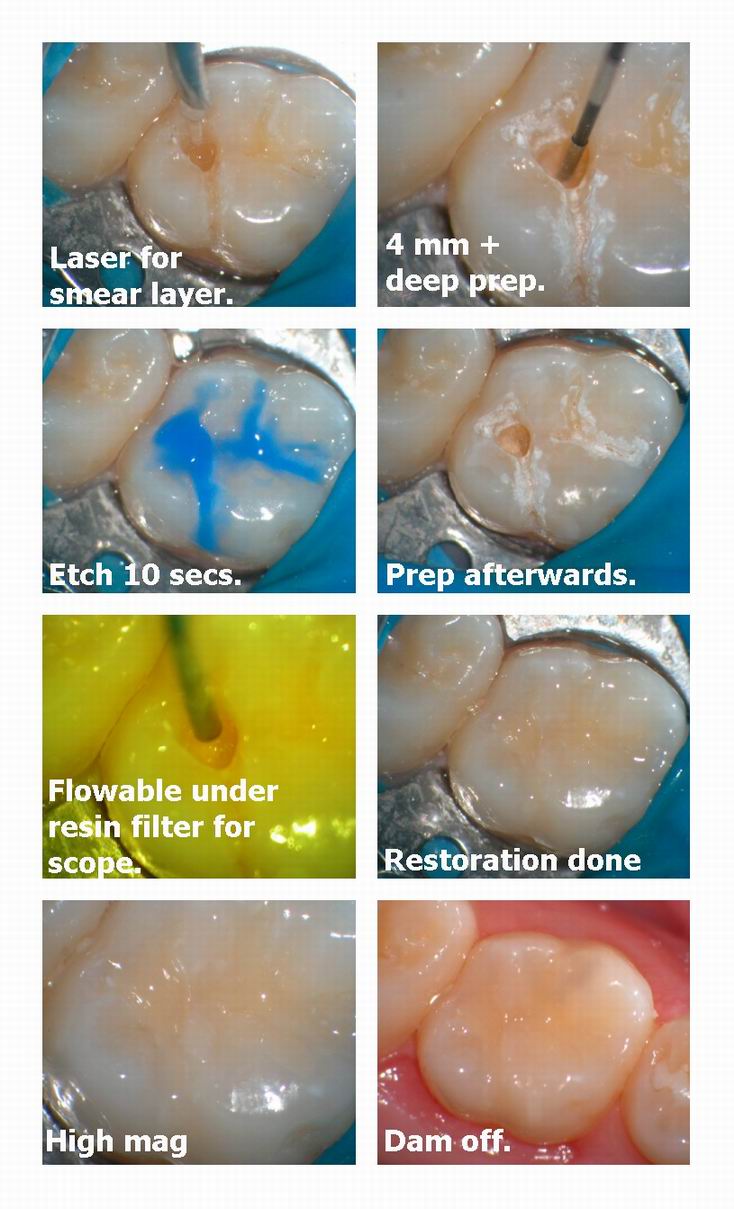
I used the Continuum laser first with a 400 micron tip to help anesthetize the tooth and to open up the groove a little bit to see where the decay went laterally. Then I use a bur (in this case a fissureotomy bur) to widen the prep to open up the access to deeper decay. Then use the laser for a minute or two to desenstize the dentin, and then a round bur for final decay removal.
To remove the smear layer I used the laser and then etched ( I know I know) , bonded and a flowable.
This one was over 4 mm deep and I still got it done without anesthetic.
Worst part was drying off the tooth after the etch.
Interesting!
Patient rated pain 8/100.
SHe hates my needle technique!!
Grin
glenn
AnonymousSpectator1week followup- lesion gone , slight cracking from winter dryness but overall good result

AnonymousSpectatorGlenn,
I’m finding I can use the high and slow speed more and more after laser anesthesia. It really speeds things up over the time it takes me to remove decay with the laser which seems to take forever- any suggestions anyone?The last amalgam removal I did was mainly done with handpieces and then the laser for etching .
( http://www.rwebstudio.com/cgi-bin….tart=20 )
My pictures aren’t that great but I think you can get an idea how deep that thing really was. All done w/o local or topical.
Glenn van AsSpectatorHi Ron: I find that soft mushy decay isnt that easy to remove with the laser. Thats when the slowspeed helps speed things up.
I also find that the laser rehydrates the decay and makes it very difficult to tell without high magnification if it is decay or solid. The caries detector gel makes a mess so you have to dry it out, use a sharp spoon , or better yet a slowspeed.
I saw your pics, and wonder how solid the dark stuff was prior to putting GI on it.
I know that in my practice I am very suspicious of leaving anything behind and will most often remove this but you know how solid it was.
It was a deep one and that was pretty big for the laser.
I think that you have to use a hybrid attack with the laser or you do risk leaving decay behind. Having said that , Mark Colonna rarely uses the drill but he does use alot of sharp spoons.
Finally, high mag helps in seeing what is decay, where is it spreading etc.
I always like to tell people my goal is to do anesthetic free dentistry where possible (not always the case) and that I will at times use a handpiece to help widen preps, and remove decay.
The laser helps anesthtetize, and remove the smear layer and remove decay especially if it isnt too huge.
Just some thoughts……….
Glenn
SwpmnSpectator[img]https://www.laserdentistryforum.com/attachments/upload/williamsa10.JPG[/img]
Hi Girls and Guys:
Take a look at this photo and grade this impression. How would you rate the impression? Terrible, acceptable, A+ or throw it away and start over?
I took this impression using the Waterlase for gingival retraction and graded it “acceptable”. My technician had no trouble reading the margins and the crown fit fine. But notice how rough and choppy the retraction looks.
Is anyone getting better results using an Erbium laser only for soft tissue retraction? If so, can you post a pic and offer suggestions? This is the best I can do with my Erbium. Are most people using Diode lasers for retraction and are the results a lot better?
Al
AnonymousSpectatorThe dark stuff was rock hard – just amalgam stain.
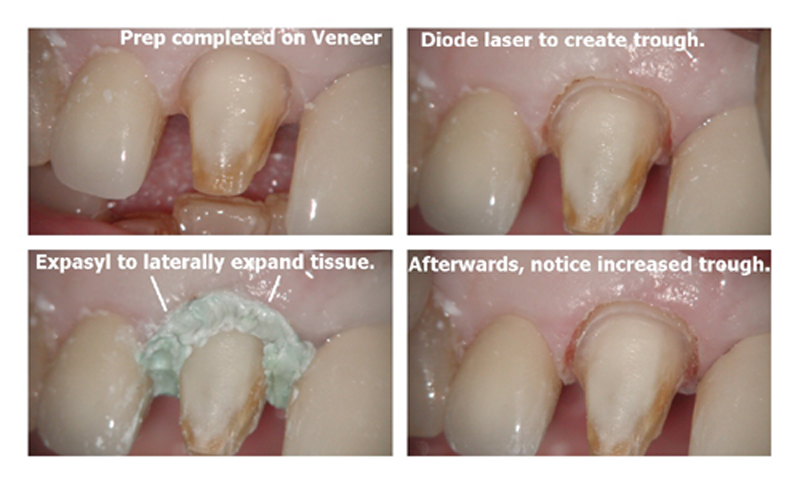
Glenn van AsSpectatorHi Al: Nice prep, I dont like the erbium for crown troughing for a few reasons……..
1. It is slow compared to the diode or argon where you can create a trough around the tooth. The erbium actually causes the tissue to be planed away whereas the dedicated soft tissue lasers create a trough.
2. It bleeds and requires a hemostatic agent.
3. It can nick your margin and cause notches depending on the setting.
I will at times put in Expasyl to laterally expand the tissue.
Check out this diode case………
Glenn
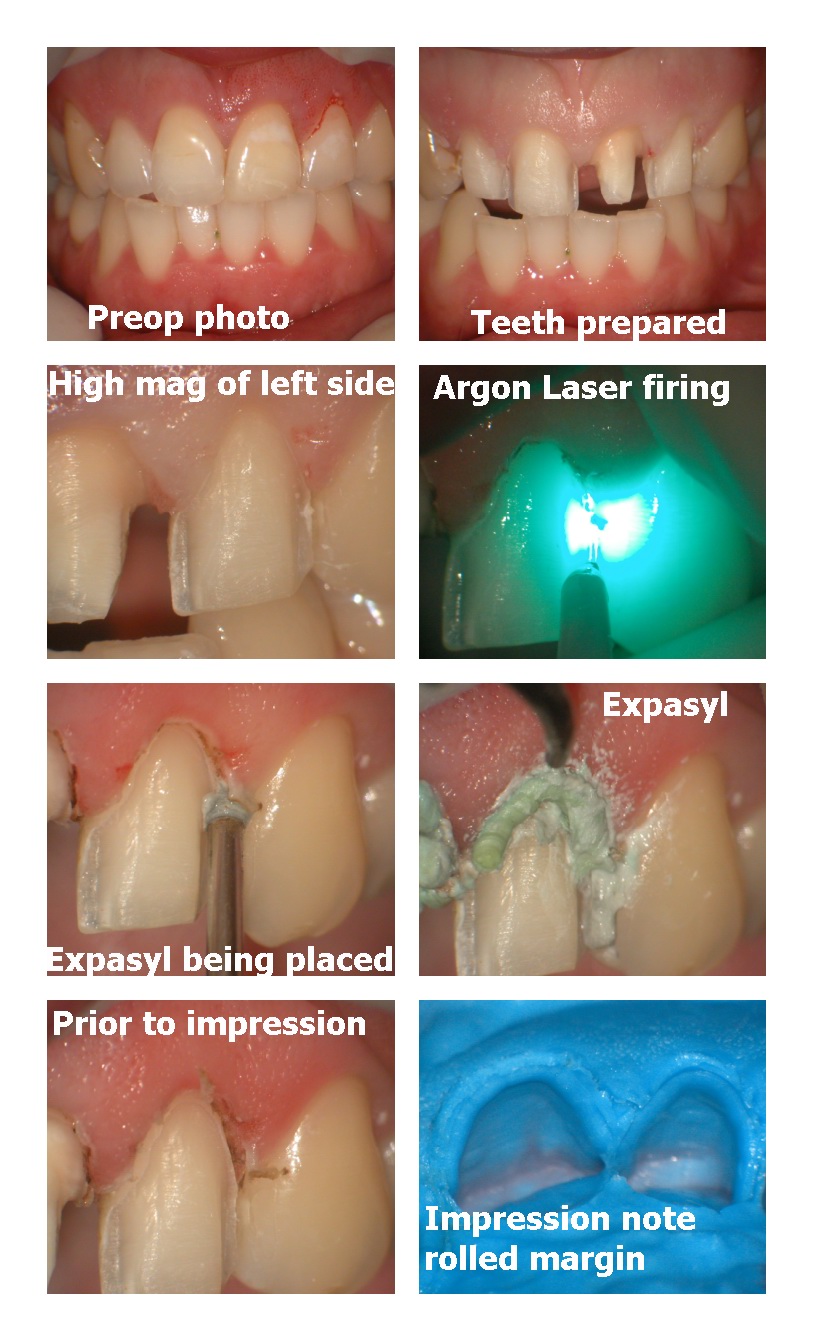
Glenn van AsSpectatorHere is a second case shot with the scope using the Argon laser to retract followed by Expasyl.
There are other less expensive ways to expand the trough but there is no oozing, a better trough and no risk of damage to the margins with the diode , argon or Nd Yag.
I havent had much success with the Erbium troughing, its the way it cuts that makes it difficult in my hands at least.
Glenn
Glenn van AsSpectatorGreat Ron………it is amazing how sometimes that Black stuff is under old amalgams…….I often try to lase it just in case it is bacteria of some sort.
Here is an example of what I mean………
A good morning to all.
Glenn
SwpmnSpectatorGlenn:
Thanks for your help and the great photos.
Basically confirms what I suspected and am experiencing down here in the Sunshine “Dangling Chad” State.
Al
AnonymousSpectatorHi Glenn,
The picture didn’t show it clearly but I also lase those dark areas. (Going to try out a new camera Friday).
This discussion also brings to mind some studies by Mertz-Fairhurst. I was wondering what others thought of these. I remember seeing an AGD video regarding this a few years back and was quite surprised as to how different this was compared to what I was taught in school. Could the ideal be -always do your best to get all the decay out but if some areas are debatable they may not be worth worrying about if they are properly sealed from the oral enviroment?
Although not scientific by any means, after successive trips to the Dominican Republic on mission trips, I have seen 1st hand teeth that were treated by spooning out the majority of decay and placing glass ionomer and composite. I was amazing to come back 2 years later and find teeth that were vital and decay arrested.
Thoughts anyone?
QUOTEUltraconservative and cariostatic sealed restorations: results at year 10.Mertz-Fairhurst EJ, Curtis JW Jr, Ergle JW, Rueggeberg FA, Adair SM.
Department of Oral Rehabilitation, Medical College of Georgia, School of Dentistry, Augusta, USA.
Changes in restorative techniques and the development of newer restorative materials have allowed for the use of more conservative cavity preparations. This 10-year study evaluated bonded and sealed composite restorations placed directly over frank cavitated lesions extending into dentin vs. sealed conservative amalgam restorations and conventional unsealed amalgam restorations. The results indicate that both types of sealed restorations exhibited superior clinical performance and longevity compared with unsealed amalgam restorations. Also, the bonded and sealed composite restorations placed over the frank cavitated lesions arrested the clinical progress of these lesions for 10 years.
Publication Types:
Clinical Trial
Randomized Controlled TrialPMID: 9448347 [PubMed – indexed for MEDLINE]
ASDC J Dent Child 1995 Mar-Apr;62(2):97-107 Related Articles, Links
QUOTECariostatic and ultraconservative sealed restorations: nine-year results among children and adults.Mertz-Fairhurst EJ, Adair SM, Sams DR, Curtis JW Jr, Ergle JW, Hawkins KI, Mackert JR Jr, O’Dell NL, Richards EE, Rueggeberg F, et al.
Department of Oral Rehabilitation, School of Dentistry, The Medical College of Georgia, Augusta 30912, USA.
The objective of this clinical study was to evaluate the long-term efficacy of placing sealed posterior composite restorations for arresting active caries. The tooth preparation for this bonded and sealed restoration was limited to placing a bevel in the enamel only, without the removal of the carious lesion. The radiographic and clinical performance of these ultraconservative sealed composite restorations placed over caries (CompS/C) was compared over a period of nine years with: 1) ultraconservative, localized sealed amalgam (AGS) restorations with no extension for prevention, and 2) traditional, unsealed amalgam restorations (AGU) with the usual extension for prevention outline form. Sealant retention with > 50 percent to 100 percent of the margins occurred in 64 percent of CompS/C and 82.5 percent of AGS restorations. After nine years the cumulative failure rates were 16 percent for CompS/C, 2.5 percent for AGS, and 17.1 percent for AGU restorations. Thus, the clinical performance of CompS/C restorations was slightly superior to that of the traditional AGU restorations. The AGS restorations were definitely superior to the traditional AGU restorations and to the CompS/C restorations in both children and adults alike. Complete sealant retention over CompS/C and AGS restorations was equivalent between children and adults (P = 0.14 and 0.74, respectively). A higher percentage of open margins in CompS/C restorations was seen, however, in children (17.4 percent) than adults (1.94 percent). This study has shown that Class I caries can be arrested by the CompS/C restoration.
PMID: 7608378 [PubMed – indexed for MEDLINE]
-
AuthorPosts